Section 1: Chair’s foreword
1.1 Paul Northcott – Independent Chair

Over the past twelve months, our members have continued to support the Partnership and the work we undertake to meet our obligations under the Care Act 2014. We have actively worked on behalf of our communities to ensure that all the organisations that make up the partnership deliver the highest standards of service for those with care and support needs and their families.
Together, we have decided to shift our priorities to become more outcome-focused. This will help us track the progress of each organisation within the partnership as they embed the changes driven by our work.
These priorities will be implemented over three years, and still recognise the value and importance of learning from the Safeguarding Adult Reviews (SARs) we have commissioned. The insights and recommendations from each review are vital in identifying not only best practice but also areas for improvement in policy and practice that we can all strengthen in the coming twelve months. Senior leaders on the Board and professionals working in each of the TDSAP subgroups have continuously monitored the progress that has been made against each of these recommendations.
We continue to foster a culture of learning, and the partnership has also ensured that we have learnt from the reviews and changes that have taken place at a national level. I continue to represent TDSAP at regional and national meetings to ensure that we meet the expected standards in safeguarding.
We continue to actively monitor performance by conducting audits and analysing data, and I have regularly met with both Directors of Adult Social Services to discuss operational delivery in this safeguarding area. Despite the challenges faced by all organisations over the past twelve months, there remains a strong desire to provide flexible services that meet the needs of those requiring support in our two counties.
I continue to be impressed by the dedication and drive of the frontline staff working across the two local authority areas, as well as the work carried out by voluntary and community organisations, without which many of these changes would never have happened.
This report highlights the hard work contributed by all agencies to the partnership over the past twelve months, and there remains a strong desire and ongoing commitment from everyone involved to make further improvements to our services.
I want to take this opportunity to thank all the agencies and those working in the voluntary sector for their valuable contribution to the partnership.
Section 2: our purpose
The Torbay and Devon Safeguarding Adults Partnership (TDSAP) is the collective name for the partners that work with the Board to safeguard adults across Torbay and Devon.
The TDSAP provides strategic leadership for adult safeguarding across Torbay and Devon and is independent, with an independent chair.
The core objective of the Safeguarding Adults Partnership, set out in section 43(2) of the Care Act 2014, is to help and protect adults in its area in cases where an adult has care and support needs and;
- They are experiencing, or at risk of experiencing, abuse or neglect; and
- As a result of those care and support needs, they are unable to protect themselves from either the risk of or the experience of abuse or neglect
The TDSAP acts as the key mechanism for agreeing how agencies work together to safeguard and promote the safety and wellbeing of adults at risk and/or in vulnerable situations. It does this by co-ordinating what each of the TDSAP members does and ensures that they do it effectively.
Section 3: our structure
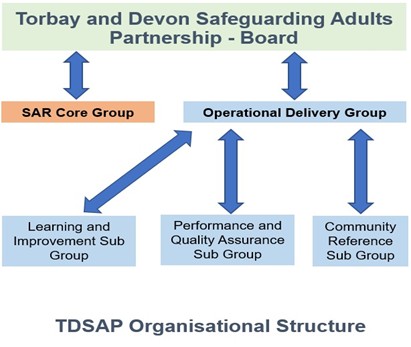
The TDSAP has established a meeting structure to undertake work on behalf of the Partnership.
The TDSAP has two groups reporting into the Board namely the Safeguarding Adults Review Core Group and the Operational Delivery Group.
Reporting into the Operational Delivery Group are three sub-groups namely the Learning and Improvement sub-group, the Performance and Quality Assurance sub-group and the Community Reference Group (CRG). These meetings will continue to be supported by the Partnership Practice Lead, Partnership Business Manager and Partnership Co-Ordinators.
3.1 Governance structure for 2024/25
Section 4: our partnership members
4.1 statutory partners
The statutory partners of the TDSAP are: Devon County Council, Torbay Council, Devon Integrated Care Board and Devon and Cornwall Police.
4.2 partners
Other partner members of the TDSAP are:
| Torbay and South Devon NHS Foundation Trust | Devon Partnership Trust |
| Royal Devon University Healthcare NHS Foundation Trust | NHS England/Improvement |
| University Hospitals Plymouth NHS Trust | Housing Representative |
| Livewell Southwest | Devon & Somerset Fire & Rescue Service |
| South Western Ambulance Service NHS Foundation Trust | Care Quality Commission |
| Department for Work and Pensions | Voluntary and Community Services Representatives |
| HM Prison Service | Healthwatch |
| The Probation Service – Devon and Torbay | The Heart of the South West Trading Standards |
| District Councils |
Section 5: safeguarding activity
The data below has been routinely monitored through the Performance and Quality Assurance (PQA) Sub Group and by Board Members to identify trends and areas for additional scrutiny. This includes variances against national and comparative area data. The data has been included in this report to demonstrate the safeguarding activity over the 2024-2025 period. Due to the timing of this report, figures may vary slightly from the Safeguarding Adults Collection (SAC) return published by NHS England.
5.1 Section 42 – safeguarding concerns and enquiries
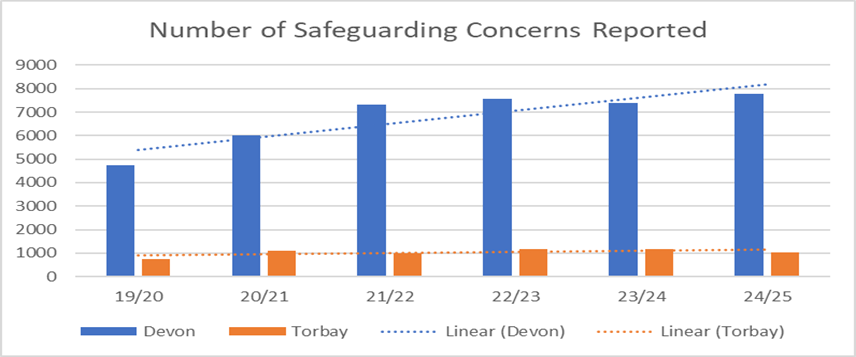
The general trend in the number of safeguarding adults’ concerns in Devon continues to be upwards, with a 5% increase in 2024-25 from 2023-24, (7773 concerns in 2024-25 from 7380 in 2023-24).
In Torbay there has been a 13% decrease in the number of concerns started for 2024-25 when compared to 2023-24, (1026 concerns in 2024-25 from 1180 in 2023-24).
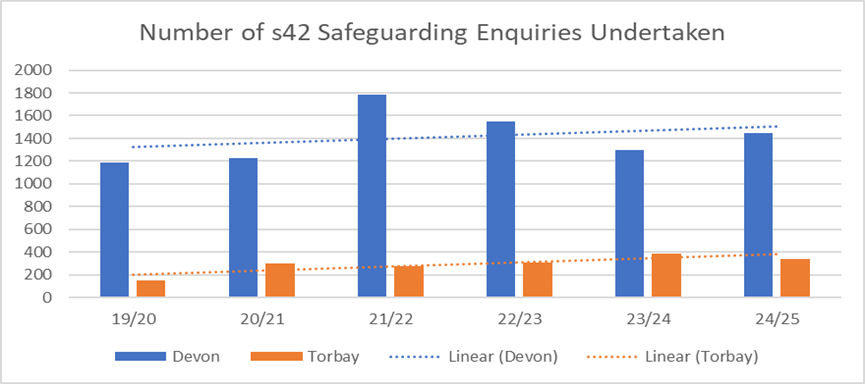
The number of s42 safeguarding enquiries (concerns that meet the criteria for further investigation) undertaken by Devon have risen from 1300 in 2023-24 to 1446 in 2024-25, an 11% increase. This may have been impacted by a recent focus on ensuring correct procedure was being followed when determining when the criteria for proceeding to enquiry had been met.
Safeguarding enquiry activity levels in Torbay have fallen by 13% from 2023-24, (340 enquiries in 2024-25 from 390 in 2023-24).
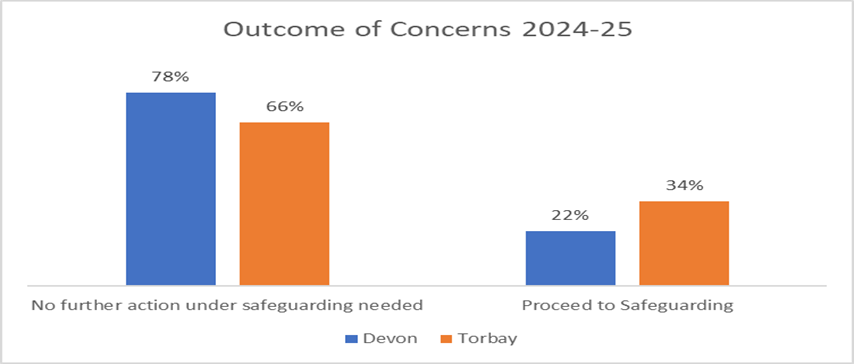
The percentage of concerns with an outcome of ‘Proceed to Safeguarding’ in Devon has been increasing. The percentage for Torbay has remained consistent with previous years.
5.2 demographics
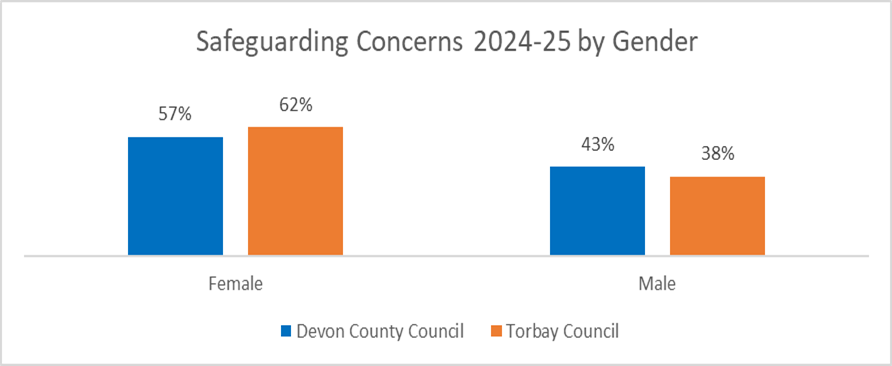
In 2023-24 in Torbay, individuals involved in concerns were 58% female and 42% male. In 2024-25 this had changed to 62% female and 38% male, (594 females, 367 males). In Devon, the percentages were 57% female and 43% male, (4417 females, 3287 males). This compares to 52% of the general adult population in England being recorded as female.
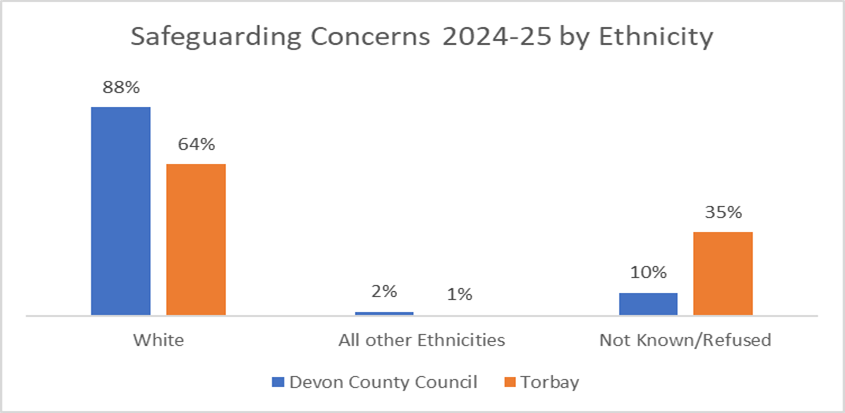
88% of individuals involved in safeguarding concerns in Devon and 64% in Torbay in 2024-25, recorded their ethnicity as white. This is very similar to the percentages for 2023-24. 82% of the population recorded their Ethnicity as white in the 2021 census. For both authorities, the percentage of concerns where ethnicity was not recorded has decreased.
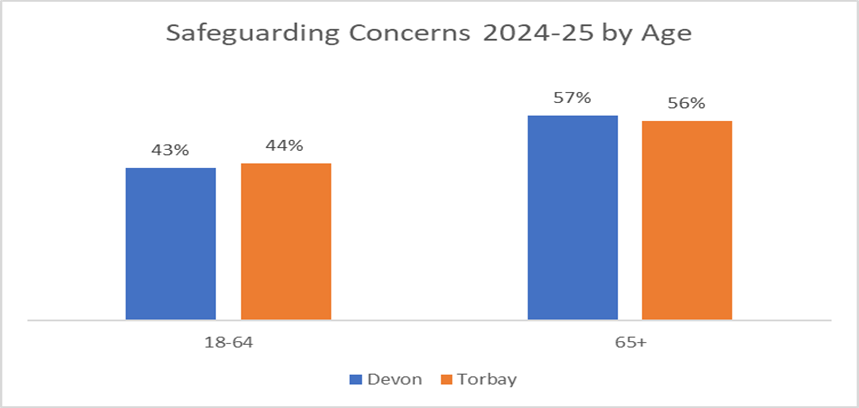
In both Torbay and Devon the percentage of concerns for those aged 18-64 has increased from 2023-24, (from 40% to 43% in Devon and 41% to 44% in Torbay).
5.3 location of risk
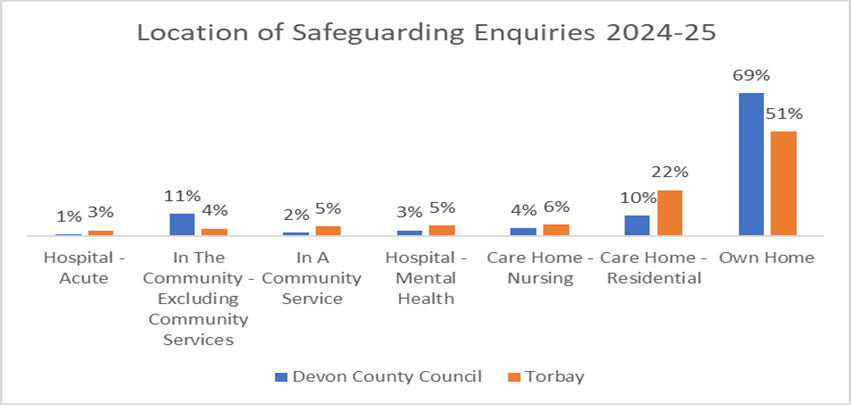
69% of enquiries in Devon and 51% of enquiries in Torbay, took place within the individuals own home, an increase for both authorities on the previous financial year.
The percentage of enquiries in Care Homes has decreased for both authorities. In Devon this was from 17% in 2023-24 to 14% in 2024-25. In Torbay the percentage has decreased from 46% in 2023-24 to 28% in 2024-25.
5.4 type of risk
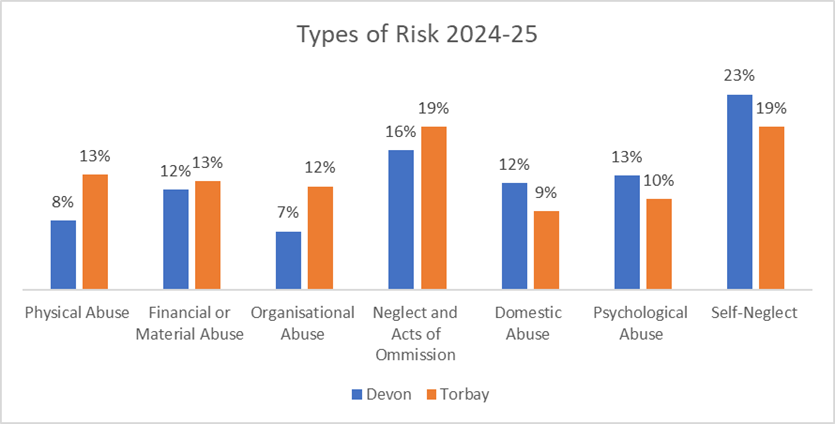
In Devon, the most common types of risk in 2024-25 were Self Neglect (23%), Neglect and Acts of Omission (16%) and Psychological Abuse (13%), the same as 2023-24.
In Torbay they were Neglect and Acts of Omission (22%), Self Neglect (19%) and Physical Abuse (13%) and Financial or Material Abuse (13%). Percentages for both Physical Abuse and Organisational Abuse had decreased from 2023-24.
5.5 making safeguarding personal
Approaches to safeguarding should be person-led and outcome-focused.
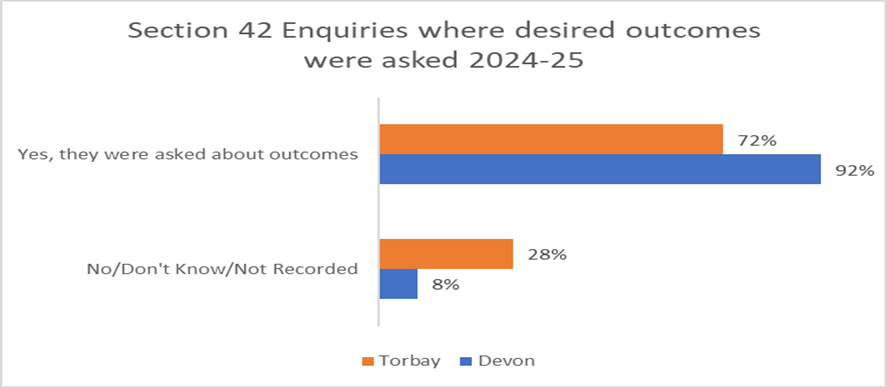
In Devon the percentage of people or their representatives asked about their desired outcomes in safeguarding enquiries in 2024-25 remains at 92%. In Torbay this has increased from 2023-24 to 72%.
Of those asked about their desired outcomes, 93% for both Devon and Torbay had their outcomes either fully or partially met.

Section 6: Safeguarding Adults Reviews (SARs) and our SAR core group
6.1 summary
Safeguarding Adults Reviews (SARs) are a statutory duty under the 2014 Care Act for Safeguarding Adults Boards to undertake. A SAR is completed when:
- an adult dies as a result of abuse or neglect, whether known or suspected, and there is concern that partner agencies could have worked more effectively to protect the adult
- an adult is still alive but has experienced serious neglect or abuse and there is concern that partner agencies could have worked more effectively to protect the adult
- Boards may also arrange for a SAR in any other situation involving an adult in its area with needs for care and support.
SARs are a way for all agencies of the partnership to identify the lessons that can be learned from particularly complex or high risk safeguarding adults cases and to implement changes to improve services.
The TDSAP has a dedicated SAR Core Group. The SAR Core Group is responsible for decision making on new SAR referrals and for managing all SARs through to completion. The SAR Core Group maintains effective oversight in relation to the progress of each SAR and reports quarterly to each TDSAP Board meeting.
The SAR Core Group membership consists of multi-agency partners who meet regularly. The SAR Core Group members include representatives from NHS Devon ICB, Torbay County Council, Devon County Council, Devon Partnership Trust (DPT), Devon and Cornwall Police and partner representatives from other organisations as required.
More specific supporting information on SARs can be found on the Torbay & Devon Safeguarding Adults Partnership (TDSAP) website here: TDSAP Safeguarding Adults Review Multi-Agency Policy
6.2 SAR activity during 2024/25
The TDSAP received sixteen SAR Referrals in 2024/25 from six different partner organisations and one family member.
Following thorough consideration of these SAR referrals, the SAR Core Group decided that five
of them met the criteria for a SAR review to take place, as defined within Section 44 of the 2014 Care Act.
The themes from these referrals include, but are not exclusive to:
- Mental Health (any support that people receive to protect or promote their mental health and psychosocial wellbeing).
- Self-Neglect (a person being unable, or unwilling, to care for their own essential needs)
- Substance Misuse (Substance misuse develops when you continue to take substances which change the way you feel and think)
- Neglect/Acts of Omission (the failure to meet individuals basic and essential needs, either deliberately or by failing to understand these).
In 2024/25 the Torbay and Devon Safeguarding Adults Partnership published Five SARs, all of which are available on the TDSAP website.
With all SAR reviews, the identified learning and SAR recommendations are progressed and embedded into operational practice. The purpose of a SAR is not to reinvestigate or to apportion blame. It is an opportunity to uncover learning for all partner agencies involved and to make changes to practices in the future.
More information is available on our website about SAR Thresholds, how to complete a SAR Referral and our previously published SARs
6.3 published SARs (including date of publication)
6.3.1 Thematic SAR: Mental health and suicide (April 2024)
A thematic review model was utilised to explore the system response during the pandemic for three men who all had complex mental health and associated difficulties. All three the men tragically took their own lives. They men were all white British and aged 59, 53 and 46 respectively.
The review focused on professional practice, challenges, system problems and constraints to practitioner efforts to safeguarding adults. Interagency working, and insight into improving responses to men in similar circumstances are encompassed in the analysis and findings of the review report.
Learning identified include:
Recommendation to review the inequalities in the funding and mental health inpatient bed provision in Devon compared to other similar populations and agreement of a way forward to address these issues.
Partner agencies to review the effectiveness of the handover process of information to improve information sharing of disclosures made by an adult prior to admission to hospital so that this information is known to treating clinicians.
Review of the escalation protocol in circumstances of mental health crisis and agency disagreement.
Review of the effectiveness of communication from acute sector to other partners including GPs regarding frequent attendees in the acute sector with self-harm.
The review acknowledged the system and practice changes since the pandemic as well as the ongoing developmental work to further address the gaps identified in the review.
The full SAR report is published on the TDSAP website Thematic SAR: mental health and suicide
6.3.2 SAR Ruth (July 2024)
Ruth, a young white British woman, was born in September 2001 with cerebral palsy, spina bifida, severe scoliosis, epilepsy and global developmental delay. She lived at home with her mother, stepfather and 5 younger siblings. Ruth was also registered partially sighted and in later years she required feeding via a Percutaneous Endoscopy Gastrostomy (PEG) tube.
As a child, Ruth was almost always smiling. She was nonverbal and had some visual impairment, and although she was not able to use Makaton effectively, she is described as having had brilliant communication and being able to let people know what she needed, making simple choices over her clothes and what she wanted to wear on a given day. Although Ruth never walked and used a wheelchair, she loved the hydrotherapy pool and other sensory/water based activities. Ruth was popular in school. She had a magnetic personality, was a very determined young lady, very giving with a calming effect on people. She loved animals, particularly riding her horse Timmy.
Ruth was a young person with a learning disability who had significant and complex needs. She and her family had been supported by a range of paediatric health professionals and she was attending a special school for children and young people with special educational needs. Her care was being provided by her parents at home, and another family member was providing breaks when needed. School was a significant source of support to the family. Ruth was defined as a Child in Need due to her disability and had an allocated Social Worker from the Children’s Disability Team.
As part of the transition from children’s to adult’s services, Ruth was entitled to an initial assessment to consider funding eligibility for NHS Continuing Healthcare, often referred to as CHC. An initial checklist assessment is undertaken by a health professional or Social Worker, then a decision is made whether eligibility is met for a full assessment by a multi-agency team of professionals. This assessment was key to ensuring Ruth’s complex needs were being appropriately met, and provision of care was in place as she transitioned.
Towards the end of 2018, there was evidence within the health records of early planning for the CHC assessment, at which point Ruth’s mother had consented to the process. A positive CHC checklist, a pre requisite to a CHC assessment, was accepted in December 2018. Ruth was then allocated to a CHC Nurse for a full assessment to take place in March 2019. This assessment was delayed, and the next reference to the assessment was in June 2019. It is noteworthy that the decision to pursue this assessment was made at a Child in Need (CIN) meeting which Ruth’s parents had not attended. It is unclear how the CHC process was subsequently shared with parents, as although it was agreed that the children’s Social Worker would follow this up, there is no record in their chronology of this CIN meeting.
Following the initial consent from Ruth’s mother to progress the CHC assessment, a key turning point was an apparent discussion between the school and parents, in which they were advised that if they pursued a CHC assessment, and health agreed to funding Ruth’s care, they would not be able to access the ongoing educational provision of their choice for her. This appears to have prompted Ruth’s parents to withdraw their consent for the CHC assessment to be undertaken. At this point there is evidence that professionals were having email discussions about the withdrawal of consent and recognised the need for careful consideration of how to address this. It was not possible to understand the context of this conversation, which is disappointing given the significant impact it had.
The review highlighted that what should have been a straight forward process of assessment, despite Ruth’s complex needs, became unnecessarily drawn out and complicated by a focus on commissioning and funding arrangements, rather than the importance of a review of health needs to ensure they could be effectively met. Consequently, there was a significant delay in provision of services. The significant delay in engaging in meaningful discussions with Ruth’s parents to understand their reason for withdrawing consent created barriers and breakdown in relationships between the parents and professionals. Ultimately, to Ruth not having in place all of the support she required to meet her complex needs in the community. In addition there was a delay in shared planning for Ruth’s transition from children’s to adult social care at an earlier stage, reducing the time available to draw together key professionals involved in Ruth’s care to undertake the Care Act assessment.
As the onset of Covid 19 led to a national lockdown, Ruth began to self-isolate at home with her family and was at home when she very sadly passed away in August 2020 at the age of 18.
Learning identified include:
Despite the unprecedented time of a pandemic lockdown telephone conversations with family were recorded as having a focus on commissioning rather than meeting health needs.
The review highlighted the importance of maintaining engagement, trust and confidence with health professionals.
Whilst various agencies assessed Ruth and shared information, it is evident that not all partner agencies played an active role in Ruth’s transition process.
It is imperative that transition planning from children’s to adult health and social care services start at an early stage and that a Care Act (2014) assessment is completed in a timely way, to avoid challenges in ensuring appropriate services are being embedded as part of the young person’s plan and support network.
It is important to have a key lead professional for the purposes of the transition from children’s to adult services especially when there are complex health needs.
Consideration should be given as to whether the key children’s lead for the young person remain involved, even if not holding the responsibility. Particularly where the children’s lead are concerned that essential information has not been conveyed to the key lead person who may be from adult services or the health service. This will ensure information sharing is effective and the new plan is progressed effectively with key areas and outlining who is responsible for those areas.
The full SAR report is published on the TDSAP website Safeguarding Adults Review Ruth
6.3.3 SAR Rachel (August 2024)
Rachel, a white British female, was born in Hastings and grew up in Bromley. She was married in 1997 and divorced some years later. Rachel has a son and a daughter; the family moved to Devon when the children were still young.
Rachel was described as ‘vibrant and loved working’ in her younger years. She worked at a local school, and she had a ‘soft spot’ for the schoolchildren. She was also described as being ‘really caring and funny’. She loved her children and is described by her daughter as a fun parent.
When the school she worked at closed, Rachel started working in social care and worked with various care agencies, supporting people in their own homes. Without access to a reliable car, she then started working in care home settings either in the kitchen or providing hands on care to vulnerable people. Various professionals have reported that in their conversations with Rachel she was proud of her job and enjoyed the work.
When Rachel’s mother was diagnosed with cancer she did not work for 3 years due to the impact this had on her. She would speak to her mother on the phone on a daily basis and her passing had a profound impact on Rachel.
Rachel had a number of health conditions including atrial fibrillation, a heart condition that causes an irregular and often abnormally fast heart rate, she had suffered with back pain, a hernia and had been diagnosed with anxiety, depression, and an emotionally unstable personality disorder at the time of her death. Her alcohol intake increased significantly following her second divorce in 2010. This affected her ability to continue working and she eventually lost her job shortly before her death. Rachel had been living in private rented accommodation and was due to be evicted from her home on 1st November 2022, due to concerns regarding the poor condition of the property.
The review identified that Rachel was well known to partner agencies and that concern had been expressed regarding her level of self-neglect and living conditions on many occasions.
Rachel was found deceased at home on the 30th October 2022. She was 51 years old. This was two days before she was due to be evicted.
Learning identified include:
The importance of sharing chronologies and social histories as a useful tool in professional analysis to ensure the identification of self-neglect where patterns may be developing and where a situation is clearly deteriorating.
Application of the Mental Capacity Act (2005) in practice, as mental capacity assessments were not completed comprehensively to assess executive function as a means to understand why things were not improving and also why partner agencies held different views about the presence of mental capacity regarding alcohol use and the deteriorating home environment.
Risk management meetings to be initiated in complex cases of self-neglect so that individual risk assessments can be shared to facilitate one joint risk assessments and the level or risk be agreed and understood by all partner agencies.
The application of a trauma informed approach, seeking to understand issues with engagement, and application of appropriate strategies to promote more successful outcomes.
Reflective supervision to include sufficient rigor considering the potential implications before ceasing involvement with an adult where concerns are ongoing. The full SAR report is published on the TDSAP website Safeguarding Adults Review Rachel
6.3.4 SAR June (January 2025)
June’s father was in the RAF which led to the family living in different countries until she was 15 years of age, and they settled in Devon. Her father would drink heavily but she described having a good childhood with her brother and sister. June disliked school and on leaving went to secretarial college. She secured good jobs as a personal assistant and legal secretary until her alcohol use increased and she was no longer able to work. Her sister died at the age of 48 due to an alcohol related illness. June never married nor had children.
June had been in a 20-year relationship with a male partner who abused her. The extent of this abuse resulted in her pouring petrol over him and setting him alight whilst he slept. June called the emergency services and was arrested and charged with grievous bodily harm. She was sentenced to 6 years in prison of which she served 3 years.
June had been using alcohol for many years alongside a history of depression and anxiety and physical health difficulties. She had a stricture which was affecting her food intake, limiting her diet to liquids and semi-liquids. June had stopped engaging with proposed treatments for her stricture and attending medical appointments; she also stopped engaging with alcohol support services.
A referral was made for an urgent mental health assessment due to the impact that June’s mental health was having on her physical health and lack of engagement with health services. An urgent safeguarding adult concern referral was also raised. There was significant delay in both these referrals being acted upon.
A 999 call resulted in June being found in bed having been unable to walk for around 5 days, looking significantly emaciated and with visible evidence of poor personal hygiene and toileting habits. June declined hospital admission and was considered to have mental capacity to make that decision. The urgent referrals made previously were followed up but with no response.
Another 999 call five days later saw June sitting on the bed in her own faeces and unable to mobilise. Again June refused to be taken to hospital and again was considered to have the mental capacity to make this decision. June said she understood that if she did not go to hospital she would die. She wanted to remain at home and sleep. Fluids were administered and a further safeguarding concern referral raised.
On the 12th June the safeguarding concern was allocated to a worker to progress. June had passed away the day before on the 11th June. June’s propensity to self-determine was a feature of her response to medical advice and treatment throughout her engagement with health partners.
June was 58 years old when she passed away.
The report highlighted several areas of good practice including:
General Practice (GP) Support
- Provided continuity of care and built a trusting relationship with June.
- Made repeat referrals for treatment and monitoring of oesophageal stricture and mental health.
- Expedited an urgent mental health assessment.
- Considered medical needs including blood tests, weight monitoring, and vitamin intake.
- Identified who was responsible for June’s food shopping and provision.
- Engaged with June’s mother to support appointment attendance.
- Raised a safeguarding referral for self-neglect due to missed appointments, poor service engagement, weight loss, mental health concerns, and alcohol use.
Torbay Hospital Gastroenterology & Endoscopy Department
- Delivered thorough and responsive care with clear assessments and management plans.
- Consultant provided personal contact details to stress urgency of treatment.
- Endoscopy booking team maintained detailed records and escalated missed appointments appropriately.
Liaison Psychiatry
- Completed a comprehensive assessment in December 2021.
- Recommended GP-led review of medication, health, and diet.
- Referred June to Together Drug and Alcohol service due to alcohol-related concerns.
Together Drug and Alcohol Service
- Conducted a detailed assessment of alcohol dependency and risk management.
- Offered welfare support including a food parcel.
- Provided more appointment opportunities than policy required to complete assessment.
- Identified safeguarding risks including partner’s role in alcohol provision and June’s debt.
- Followed up with GP to prompt a formal safeguarding referral.
- Made welfare calls reinforcing the need for GP engagement.
- Maintained a dedicated safeguarding lead for each Devon area.
Community Mental Health Team
- Advised that the GP should initiate a safeguarding referral without waiting for mental health assessment completion.
Police
- Recorded comprehensive safeguarding risks on the ViST form in December 2021.
Ambulance Service
- Signposted mental health services following June’s overdose.
- Raised a safeguarding concern, acknowledging self-neglect and recent GP referrals for mental health support.
Learning identified includes:
Communication in the form of direct conversations between agencies when there is a deteriorating situation and need for a priority response. This can reduce the risk of a mismatch between the expectations of what constitutes an urgent referral for support.
The importance of consideration of an assessment under Section 9 of the Care Act (2014) when it appears that an adult has needs for care and support.
The need to consider a Mental Health Act (1983) assessment if someone is at risk of seriously harming themselves or others.
Professionals to consider other influencing factors, such as alcohol dependency, mental health challenges, or deteriorating physical health, that may impact on an adults ability to make informed and capacitated decisions when cancelling, declining or missing health appointments.
Professionals may be hesitant to intervene when an adult at risk with capacity appears to be making unwise decisions, due to a common misunderstanding of the Mental Capacity Act (2005). This misconception – that individuals have a ‘right to make unwise choices’ – can lead to inaction. However, it is unhelpful and potentially harmful to assume that someone who is self-neglecting is necessarily making a capacitated decision.
The full SAR report is published on the TDSAP website Safeguarding Adults Review June
6.3.5 SAR William (February 2025)
William, a white British man, was born in Wiltshire and described as a quiet reserved young man who often chose to spend time on his own. He was popular with others and enjoyed reading or watching films. From his early to mid-thirties, he returned to live with his parents and worked as an accountant with a company linked to a car manufacturer. William never married or had any children. He moved to Devon at the same time of his retiring parents when he was in his mid-forties and purchased his flat. He was part of his local community and worked as a postman. He was immensely proud of this and in later years would often talk about his time as a postman. His father passed away in 1987 and his mother, who would do everything for William, passed away in 1994.
Following the death of his mother William immediately started to withdraw. He rarely answered his phone and had minimal communication thereafter with his surviving brothers. His brothers visited him as they were worried about lack of contact approximately 14 years before his death and they were shocked by the state of his property. It was described as dirty with papers piled halfway up walls.
Practitioners described William’s flat as having newspaper all over the floor, some of which dated back to 2008, plastic cartons would also be stacked in a central place. When speaking about his home environment William would give responses like “I don’t know how it gets like this”, “I clean it up and then it just gets messy again”.
All his personal paperwork and books were stacked neatly. William loved to read, and he did not want to get rid of anything he had already read or might want to read in the future. Things that were important to William appeared well organised. On the last home visit by a relevant partner agency, it was noted that there was water pooling on the floor. When asked about it, he gave a nonchalant response as if he was avoiding it or hoping it would fix itself. William’s home was deemed to be a high fire risk from 01 July 2021. A smoke alarm was provided, and a safeguarding concern was raised.
The clothes that he wore were extremely worn and threadbare most likely dating back to when his mother was alive. This included a hat he would wear that had worn down to just a rim, torn trousers and no soles on shoes. William also developed a large scrotal hernia which was inoperable and would often be visible due to his torn trousers which would not afford protection. There is one record of William being asked to leave a community environment due to his appearance.
On one occasion, William said a stranger put money in his hand thinking he was homeless. William appeared genuinely surprised by this and could not understand why someone may have thought this. William was quite a wealthy man, so his physical appearance was not dictated by money. He would spend up to £600 a month eating out in local café’s saying he did this to support local businesses.
William consistently expressed a reluctance to engage with professionals or consider offers of care and support saying he was fine and well fed as he ate out. However, throughout the timeline of this review, concerns from people within his community were raised. These came from a genuine concern for his welfare where he was described as a very ‘nice and compliant person’. One community report for example highlighted that William would regularly cause public disturbances at night from his property balcony, but the concern contact was made from a welfare stance.
One of William’s brothers passed away in November 2022 shortly before William’s death in December 2022. His surviving brother could not get hold of William and through social media he received information from the local community that William had been seen looking really unwell, scruffy in appearance and his movements were described as ‘shuffly’.
After William’s death at the age of 79, his brother visited his property and described being ‘truly shocked’ by the state of the property. The rooms were piled high with magazines and papers, there was dust and cobwebs everywhere and a bath was brim full of milk cartons and cans. There was no bed as such, just a mattress and a sheet. The review highlighted that new concerns for William’s welfare were raised in June 2022 which also indicated a possible mental impairment. Although a number of contacts were made with William by partner agencies, there was a lack of appropriate multi agency working and information sharing to safeguard William.
Learning identified includes:
The importance of practitioners actively appraising themselves and reflecting on, Safeguarding Adults Reviews information disseminated by the partnership. This is a vital component of maintaining ongoing professional development and embedding learning review information into practice.
The need for all practitioners to be aware of how to initiate effective multi agency meetings and be familiar with their internal escalation processes in response to any barriers that may arise.
Where there is a reason to doubt an adult’s mental capacity and completion of an assessment is paramount in the assessment of risk, all relevant professionals should prioritise their attention to the completion of a Mental Capacity Act 2005 assessment.
The importance of relationship based practice when engaging with adults in circumstances of self-neglect and to promote effective handover and introduction of new practitioners as part of best practice in case management where it becomes necessary for a change of practitioners due to sickness, leave or the cessation of a practitioner’s employment.
Relevant partners and their commissioners should be clear on their mechanisms for front line practitioners and managers to escalate unmet need identified in self-neglect cases and ensure that they receive effective feedback to understand what if anything is being done in response.
The full SAR report is published on the TDSAP website Safeguarding Adults Review William
Section 7: TDSAP sub-groups
7.1 community reference group
The Community Reference Group (CRG) has worked closely with voluntary, community and social enterprises to facilitate and promote co-production. The CRG has achieved this by working in partnership with members of the CEG and the people that they support.
The CRG has raised awareness of adult safeguarding throughout the year, especially during Safeguarding Adults Awareness Week in November. The CRG produced a schedule for the week and assisted with dissemination of materials via social media and their own networks.
A main focus of the CRG has been to improve the wider awareness of safeguarding adults within the ‘perceived harder to reach’ communities of Torbay and Devon. This has been a challenge to achieve and work continues alongside Living Options and the organisations involved with the CRG.
Examples of the co-production work of the CRG can be seen within the TDSAP leaflets, posters and easy read guidance documents produced for the TDSAP and its members to utilise. These are available on the TDSAP website by clicking here and here
The CRG works openly and inclusively, keeping adults with lived experience of safeguarding and carers at the heart of all it does. Via the groups representatives, the CRG ensures it listens to the views of adults with lived experience of safeguarding, their Carers and relevant members of the public.
The CRG reports to the Operational Delivery Group (ODG) on a quarterly basis with a progress report provided to the ODG each quarter.
The Group is made up of people from organisations who represent adults, or from relevant members of the public recruited for their insight and interest.
In 2024 the CRG agreed to undertake a review of its functions and purpose. Following this review, a rebranded and refocussed group was agreed. This new focus ensures a clear line of sight to raise awareness and understanding of safeguarding adults within ‘perceived harder to reach groups’, diverse communities and ethnically minoritized people. This coupled with a continued investment in current membership will ensure a clear focus on co production and co design. The refreshed group falls in line with the TDSAP Strategic Priorities for 2025-2027.
The new group is named The Community Engagement Group (CEG). An update on the progress of this group will be included with the TDSAP annual report for 2025/26.
7.2 learning and improvement sub-group
The Learning and Improvement sub group has over the last year continued to focus on driving learning and practice improvements across partner agencies resulting from the recommendations from Safeguarding Adults Reviews, and other identified focus areas for learning and development.
During the last year it was agreed that active SAR action plans be moved from this sub group back to the SAR core group to ensure that the responsibility for ensuring completion of SAR recommendations sits with the SAR core group who has responsibility for agreeing the SAR recommendations before sign off at TDSAP Board. This further ensures that the Learning and Improvement sub group’s focus remain on learning and practice development.
Areas of development include:
- Review and refresh of TDSAP Safeguarding Adults Level 1 e-learning training – The sub group steered the review of the safeguarding adults level 1 training offer.
- Training procurement – Representatives of the sub group supported the procurement process for TDSAP training aimed at Devon provider services. Two new providers have been commissioned to deliver the Safeguarding Adults training and Mental Capacity Act (2005) training respectively. New training dates for course delivery have been agreed and made available on the TDSAP website.
- Review of the TDSAP Training Strategy – The training strategy review was previously paused whilst awaiting the publication of the updated intercollegiate document (Adult Safeguarding: Roles and Competencies for Health Care Staff). The review of the TDSAP training strategy is now underway.
- Unpaid Carers and Safeguarding – Representatives of the sub group supported the development of a TDSAP web page on ‘Unpaid Carers and Safeguarding’ alongside a 7 minute briefing to raise awareness of the voice of Unpaid Carers who often choose to continue to care, even though doing so, may put them at risk of abuse or harm. The briefing highlights the importance of ensuring that Carers have an opportunity to talk in private about the impact that caring may have on them and for practitioners to consider what support may be needed and not to assume the impact ‘can’t be that bad’. Unpaid Carers and Safeguarding
- Safeguarding Easy Read – Development and publication of a safeguarding Easy Read booklet and safeguarding Easy Read fact sheet. Easy Read resources
- New practitioner guidance to support partnership working with adults who present with self-neglect behaviours and adults who present with hoarding behaviours – Practice guidance were adopted and adapted, inclusive of local learning from SARs, to support partner agencies across Torbay and Devon when working with adults who may display hoarding or self-neglect behaviours. Self-neglect and hoarding guidance
- Development of a TDSAP safeguarding leaflet and poster – Learning from reviews highlighted that adults often do not understand the safeguarding process and what to expect. The sub group led on the development of a TDSAP leaflet and poster which will support the work of partners in raising awareness of adults at risk of abuse or neglect. TDSAP resources
- Development of a TDSAP newsletter – the sub group has been driving the ambition to develop a quarterly newsletter to raise awareness of the work of the partnership, share training and learning opportunities.
- Development of SAR practitioner briefings – The sub group continue to support the development of practitioner briefings to highlight the learning from Safeguarding Adults Reviews which are then circulated to all partner agencies to ensure the learning is shared widely and action taken to embed the learning into practice. Sub group meetings have included a focus on obtaining assurance from partner representatives on how these practitioner briefings are shared, what was working well and what could be improved to ensure this learning is shared and embedded in practice.
The Learning and Improvement sub group continues to monitor closely the training offer and uptake from partners, including the private, voluntary and independent sectors.
7.3 performance and quality assurance sub-group
The Performance and Quality Assurance (PQA) sub group supports the Torbay and Devon Safeguarding Adults Partnership to take a strategic overview of the performance and quality of safeguarding activity across Torbay and Devon.
The Quality Assurance Framework is underpinned by the Care Act 2014 safeguarding principles. This includes the expectation that learning from quality assurance will be shared with partners to bring about positive change to practice and to improve outcomes for adults with care and support needs and their carer’s. The group meets quarterly, has clear terms of reference and a robust quality assurance framework and guidance which has been recently reviewed to support a renewed focus for the next 12 months. The framework sets out the focus for the PQA subgroup measured against the new TDSAP strategic priorities for 25 – 27 to include further self-assessment audits, themed audit, qualitative and quantitative feedback from all partners and embedding learning from SAR’s .
The PQA supports the safeguarding Partnership to look at what we do, how well it is done and what difference we can make to improve and enhance operational systems and processes.
In 24 – 25 the PQA completed a comparison review of prior and current Torbay and Devon SAR’s in order to identify recurring themes and understanding what further work needs to be undertaken to ensure that learning is embedded within safeguarding practice across the safeguarding footprint. The review has led to recommendations for enhancement work within the SAR Core Group to ensure that SAR recommendations are clear and measurable.
During 24/25 the group undertook TDSAP Safeguarding Assurance self-assessment audit for those with lived experience of safeguarding which evidences how multiagency partners support those with lived experience to have their voice heard and supports quality assurance of the safeguarding process. Partners contributed to the audit and have provided assurance and evidence to the TDSAP Partnership Board of continued multiagency engagement by all partners who continuously work to improve involvement and engagement with people who are experiencing safeguarding processes. Partners have also been requested to, and have shared at the quarterly meetings, details of agency internal audits that have given further assurance regarding safeguarding activity across the TDSAP footprint. The Partnership agreed their new Priorities in December 24 and the annual audit for 24/25 was deferred in order to carry out a baseline audit in year one, against the new TDSAP priorities.
The sub group regularly reviews safeguarding adult performance audit data which supports the identification of areas where further assurance focus work is required. An example of that would be the focus of the group regarding self-neglect practice improvements in 24/25 which links closely with the Partnership’s strategic priorities regarding embedding the learning from SARs and improving the outcomes for people with needs for care and support by finding the right solution for them.
The subgroup continues to provide assurance that the Partnership and its constituent partner agencies have effective systems, structures, processes, and practice in place to improve outcomes and experience in the context of safeguarding adults at risk.
7.4 operational delivery group
The TDSAP Operational Delivery Group (ODG) meets quarterly and is responsible for delivering the activities to support the TDSAP Strategic Priorities.
The group also considers safeguarding adults multi-agency practice, process and systems across Torbay and Devon to ensure that there is effective communication and quality working practice in place. The ODG does this to ensure that members of the public and people who draw on care and support are protected from potential abuse and harm.
A key purpose of the ODG is to ensure subgroups report directly to the ODG on progress of priority activities. In 2024-2025 the ODG retained oversight of the restructure sub-group arrangements leading to the newly formed Quality Assurance and Improvement Group and Community Engagement Group.
This has been an active year for the ODG. The TDSAP training strategy has been updated and revised to ensure consistency of approach against national benchmarks. Revised self-neglect and hoarding guidance has been updated and published to reflect additional learning from SARs.
In addition, the self-neglect task and finish group led on activity such as the June 2026 self-neglect conference. Another task and finish group led on the test and learn pilot of Multi-Agency Risk Management Meeting (MARMM) systems and processes, leading to a clear timeline for full implementation across the partnership in 2026.
We strengthened our links with local and regional homeless and rough sleeping partnerships receiving regular updates from colleagues within these arrangements and received information of the Devon Safeguarding Children’s (Devon SCP) thematic review of child to adult transition services. The TDSAP also developed new public and partnership information posters and leaflets and further enhanced information accessible on its public website.
Section 8: summary of partner achievements during 2024/25
Below is a selection of the key partner achievements, in relation to safeguarding adults, during the year:
8.1 Devon County Council (DCC)
DCC has conducted comprehensive qualitative and quantitative audits which has helped to identify key areas for improvement in ensuring compliance with statutory safeguarding responsibilities. We have worked to refine our systems and processes whilst strengthening workforce support to embed these practices effectively. This ongoing work ensures that the adults we support are safeguarded from abuse and neglect, while empowering them to make informed choices. That the safeguarding decisions we make support adults to make choices that balance risks with positive, choice and control in their lives.
DCC has recommissioned its training on the Mental Capacity Act (2005) and Safeguarding Adults, placing a stronger emphasis on embedding trauma-informed practice throughout the organisation. Two new specialist providers have been engaged to deliver this enhanced training. Additionally, a new e-learning module on modern slavery has been developed to further support staff awareness and understanding
DCC has strengthened its SAR governance processes by improving the allocation of actions to designated owners and enhancing the monitoring of their completion and sign-off within our internal safeguarding governance group. These improvements have significantly reduced the time actions remain open and have ensured more timely and effective responses to learning identified through SARs.
8.2 Torbay and South Devon NHS Foundation Trust (TSDFT)
The responsibility for adult safeguarding duties in Torbay is delegated from Torbay Council to Torbay and South Devon NHS Foundation Trust.
This has the benefit of providing a joined-up service in our safeguarding system by providing timely health and social care responses to the concerns we receive.
Torbay adult social care continues to receive qualitative feedback from people who experienced a safeguarding response through independent quality checkers. Feedback continues to be very positive. People tell us that they feel included and listened to, that the process is fully explained to them and that they value the safeguarding response. All feedback is reviewed and is used to help improve our service and how we work.
Within our health regulated services, the Friends and Family Test (FFT) remain an important feedback tool that supports the principle that people who use the NHS should have the opportunity to provide feedback on their experience. People are asked if they would recommend the services they have used and offers a range of responses. When combined with follow-up questions, the FFT provides a method to highlight both positive and negative patient experience.
In the past 12 months, our health services safeguarding team has focused on developing resources and training available to staff. For example, we have changed the way we deliver safeguarding adult training to make it more accessible for all staff. We also commissioned an Independent Mental Capacity Act audit which enabled us to build on our strong foundation for Mental Capacity Act training by delivering and designing targeted training to enhance staff knowledge and confidence. Other activity includes strengthening the presence of the Independent Domestic Violence Advocate within clinical teams. Within adult social care services, we have responded to safeguarding adults reviews published by the Torbay and Devon Safeguarding Adults Partnership (TDSAP), ensuring there is a continued focus on embedding learning. Examples include introducing practice exercises into training (Self Neglect) and enhanced multi-disciplinary oversight arrangements (SAR Hermione). We also commissioned an Independent Deprivation of Liberty Safeguards audit from which we have implemented a new operating model to facilitate more effective use of available resources. We continued to enhance our use of data to monitor safeguarding activity and respond to potential areas of risk.
8.3 Devon and Cornwall Police
As part of Victim Focus Week we held our first ‘Lived Experience’ conference to understand and learn from the trauma of victims of rape and serious sexual abuse. Survivors and family members were invited to share their experiences – both good and bad – of the criminal justice system. The event highlighted the importance of giving support to victims of domestic abuse when a perpetrator is being prosecuted.
Missing & Suicidal TextSafe is an innovative suicide prevention service, delivered by Missing People and Samaritans. This crisis support service is focused on a critical moment for preventing suicides when people have gone missing with suicidal intent. Devon and Cornwall police have signed up to the suicide TextSafe process to build a vital bridge between the missing individual and support networks. It complements our investigative work by engaging the person emotionally and encouraging self-rescue, sometimes leading to safe resolutions without the need for escalation.
We have significantly improved our Domestic Abuse arrest rates following clear messaging from leaders to ‘arrest to protect’. Arrest must be considered for every DA crime within the framework of Code G of the PACE Codes of Practice where one or more of the necessity criteria applies. As a result of a continuous focus on performance and consistent messaging and training we have now increased our arrest rate for DA to over 50%.
The DARA risk assessment tool has been launched for frontline police responding to domestic abuse and has been developed to ensure that first responders are supported to make people safe by helping them recognise patterns of controlling and coercive behaviour more easily and as early as possible. Officers are required to use professional judgement and officer’s observations to make a primary assessment of risk of harm to the victim.
8.4 Devon Partnership Trust
Devon Partnership Trust (DPT) continues to be a proactive member of the Board and its sub groups.
In 2024/2025, clinicians within the Trust raised a total of 1,113 safeguarding concerns on behalf of our patients to the Local Authority and some 310 safeguarding adults enquiries were caused out to the Trust (under s42(2), Care Act). For 29% of these enquiries, the primary domain of abuse or neglect identified was self-neglect and for 18% of enquiries it was domestic abuse.
DPT continue to ensure all registered clinicians and practitioners complete level 3 safeguarding training in both safeguarding children and adults.
Key initiatives in the last year have included:
- Ongoing collaboration with partners regarding the implementation of Right Care, Right Person and the development of a Mental Health/Police Operational Delivery Group
- Maintaining a focus on Sexual Safety; with the development of bespoke sexual safety training for staff.
- Maintaining an offer of safeguarding supervision to staff – with over 4000 engagements by staff in safeguarding supervision. Safeguarding Supervision is delivered solely by members of the Central Safeguarding Team who have all completed training in restorative safeguarding supervision.
- Executive Board continues to be updated and provided with assurance on safeguarding through:
- Weekly safeguarding reports
- Integrated Safeguarding Committee and the work of its associated subcommittees
- The internal Trust Safeguarding and Legal Bulletins delivered to staff bi-monthly – these provide staff with access to learning from Safeguarding Adults Reviews and complex safeguarding enquiries
- Learning and reports from our Executive Complex Case Forum
- Learning and reports from our Ethics Committee
8.5 NHS Devon
Following the NHS Devon restructure due to budgetary constraints in 2024, reductions in personnel were made to the team. Though the team has had to revise the way we work across the health and social care system, the team continues to provide consistency to the safeguarding Partnerships and to keep safeguarding a priority though there are continued extreme pressures on health systems. An example of this has been the lead role the team took with the implementation of the Right Care Right Person National Police initiative, which is a revised operational model that changes the way the emergency services respond to calls involving concerns about mental health, ensuring the voice of those most vulnerable in the healthcare system were considered. The NHS Devon MCA lead continues to organise and chair a Devon wide network that supports MCA leads in Trusts to share practice and resources and led on a self-assessment audit of Healthcare services in Quarter 4 24/25.
In January 2025, following consultation, the NHSE National Safeguarding Steering Group launched updated versions of a range of assurance protocols with the aim of supporting ICBs to have a consistent and sustainable approach with their safeguarding accountability and assurance function in line with the Safeguarding Assurance and Accountability Framework (SAAF) 2024. Protocols include Child protection Information System, Domestic Homicide reviews, Female Genital Mutilation, Modern Slavery and Human Trafficking, Safeguarding Child Death Reviews, Domestic Abuse Sexual Violence, Serious Violence and Prevent. Ensuring benchmarking of NHS Devon practice against each of the protocols is comprehensive and ongoing.
Following NHS Devon taking on delegated responsibility for dental, ophthalmic and pharmaceutical services (POD) in April 2023 the team have continued to work closely with the Collaborative Commissioning Hub to support the design and delivery of POD services and supported the Local Authority Safeguarding teams in navigating the new commissioning structure.
The NHS Devon Serious Violence and Trauma Lead (SVTL) joined the NHS England Domestic Abuse Team task and finish group to contribute the Home Office violence against women and girls (VAWG) strategy. The SVTL was also invited to join a Home Office roundtable on health and domestic abuse chaired by minister Jess Phillips and Baroness Merron in which Devon was described as an exemplar for other areas. She continues to lead and support DASV improvement work across the healthcare system in Devon such as supporting to ensure all acute Trusts have Independent Domestic Abuse Advocates and the General Practice Interpersonal Trauma Response Service (ITRS).
8.7 Royal Devon University Healthcare NHS Foundation Trust
Our staff continue to identify safeguarding issues and the numbers of ‘concerns raised’ with Devon County Council’s Safeguarding team increase month on month. The positive safeguarding actions to support our patients is achieved because we provide education and training on all areas of safeguarding and a particular focus on self-neglect, seen through a lens of trauma informed practice. All our services demonstrate a continuous commitment to promoting learning from safeguarding reviews and other learning reviews. These have been embedded into our learning systems so that Staff can capture their safeguarding learning using an electronic log.
The MCA team has successfully implemented a 7 day DoLS review process which ensures that any of our patients who are deprived of their liberty under the DoLS framework are assessed to ensure this remains appropriate. The team has worked with clinical areas to reduce restrictive practice in line with the Use of Force Act (2018). We have also successfully supported surgical areas to provide care and treatment in line with the MCA (2005) to patients with a Learning Disability. The Royal Devon has fully adopted the Sexual Safety Charter which provides support and to staff and patients. We are committed to our roles and responsibilities in the Domestic Abuse Sexual Violence Programme. Domestic Abuse is a thread through all of the clinical areas including the Care Groups. We continue to work with partners to improve our recognition, response and support of our patients in all aspects of safeguarding. There has been a corresponding increase in disclosures from patients and staff which has resulted in safety plans and support being offered.
8.8 Probation Service
We have linked adult safeguarding training to pay progression for staff so we can ensure that this important learning is prioritised. We have 100% compliance rate for people having undertaken their safeguarding adults training.
We have held quarterly safeguarding briefings for all staff to ensure learning from Safeguarding Adults boards is disseminated. During these meetings we review learning from Safeguarding Adults Reviews and ensure that staff are aware of any upcoming training opportunities.
This year we have increased the number of home visits we complete in a timely way to ensure that we see people in their environments. This is increasing our awareness of adults who are hoarding or self-neglecting and staff are aware of how to raise concerns through appropriate channels in these situations.
8.9 Devon and Somerset Fire and Rescue Service
Work has been done to establish Devon and Somerset Fire and Rescue Service’s internal Safeguarding Steering Group and Safeguarding Board to provide more robust governance arrangements in relation to all aspects of safeguarding across the service.
The implementation of the internal Safeguarding Steering Group and Safeguarding Board has also supported governance arrangements around SARs and other reviews. This will ensure that learnings and recommendations from SARs are embedded within the service and the progress of which will be monitored. This work has also been linked with the service’s wider work around the Safeguarding Fire Standards and will help us achieve the desired outcome of “being a service that actively promotes the Safeguarding of those in its community and its employees and volunteers,” and to be a service that “collaborates appropriately with others to ensure a coordinated approach to Safeguarding.”
DSFRS’s internal safeguarding team have been carrying out a programme of engagement with all fire stations and operational staff to find out how we can better support staff in aspects of safeguarding, including recognising concerns and raising referrals to our internal team. This proactive approach has been successful in achieving organisational learning and increasing the safeguarding awareness and knowledge of our firefighters. We have seen a very positive level of engagement from the crews and will be collating our learnings and using it to make improvements to our referral process and referral form to better capture risk information with the aim of improving the quality of the referrals we make into social care and other agencies. This engagement will be further supported by further training and communications around safeguarding and the development of a service wide training plan.
8.10 Livewell Southwest
Livewell has now appointed a lead for domestic abuse and sexual violence and we have been working in partnership with both the local authority and our VCSE partners to look at how we can increase awareness amongst our clinical and professional workforce. We have introduced mandatory questions into our main electronic patient record system, which will ensure that domestic violence is explored as part of our core assessment. We are also reviewing our training requirements to ensure that our staff are both competent and confident to discharge the vital role they play in helping survivors of domestic abuse and sexual violence seek help.
Building on the improvement work started last year with Plymouth City Council, we have now been through a CQC inspection, which will include a review of the adult safeguarding pathway. We have been exploring ways of including the voice of the person in our improvement work, as well as looking at our data and challenging ourselves as to how we are assured that our safeguarding interventions are adding value to people’s lives and how we could evidence this. Our principle social worker has also expanded our casework audit work, which means we now have better information about the areas of practice that require additional support and focus, as well as the areas where our social workers are providing exceptional support to our most vulnerable citizens.
Finally, we are starting to explore how we can make safeguarding more integrated, across our health and social care teams, recognising that it is very often the clinician who knows the person best who is best placed to support with initial discussions and to explore the person’s wishes and preferred outcomes. This work is in its early stages but as a result of the successful co-location of mental health and safeguarding teams, we have already started to test the benefits of closer working relationships.
Section 9: TDSAP priorities 2025/27
Under the Care Act 2014, the TDSAP must develop and publish a strategic plan that clearly sets out how it plans to achieve all its statutory objectives.
In developing this strategic plan, the partnership has worked closely with partner organisations and sought input from community groups, to develop a set of priorities that best reflect the needs of Torbay and Devon.
The work of the partnership is not exclusive to these priorities: flexibility is a key characteristic of the TDSAP and priority will also be afforded to urgent themes and risks that present themselves throughout the plan period.
The TDSAP Board agreed these three strategic priorities for the period from 2025 to 2027.
- To seek assurance from partners in relation to practice improvements in key risk areas
- To seek assurance from partners that learning from SARs is embedded into practice
- To improve awareness, engagement and inclusion
How will we monitor and ensure delivery:
- The TDSAP Business Activity Plan monitors and reviews the development, progression and delivery of the actions that support these Strategic Priorities
- The Operational Delivery Group holds the Business Activity Plan and reports on progress to each TDSAP Board meeting
- We will regularly monitor and assess the safeguarding data and performance to inform future thinking and direction of travel
- A yearly Annual Report is produced that describes the activity undertaken by the partnership