This guidance went live on 9 March 2026 across the Torbay and Devon partnership footprint.
1. Introduction
The Care and support statutory guidance (July 2025) states that ‘agencies should implement robust risk management processes in order to prevent concerns escalating to a crisis point requiring action under safeguarding adult procedures’.
Safeguarding Adults Reviews (SARs) commissioned by the Torbay and Devon Safeguarding Adults Partnership (TDSAP), in particular SAR Erik and SAR Rita, highlighted the need to develop a multi-agency risk management framework to enable a collaborative approach for partner agencies when presented with adults who may engage in, or find themselves in, circumstances of high risk.
Partner agencies utilise their own internal mechanisms to identify, record and assess risk. However, this information is often held on separate recording systems, which may not provide a holistic overview of an adult’s circumstances and the levels of risk they are presented with.
Sharing of high risk information held by partner agencies enables a richer picture and the development of a shared, understood and agreed risk assessment which in turn then promote the shared responsibility of partner agencies to take appropriate actions in addressing those risks.
It is acknowledged that the geographical footprint comprising Torbay Council and Devon County Council consists of a number of districts, several Integrated Care Board Local Care Partnerships and policing sectors which consequently present challenges in delivering consistency in the appropriate sharing of information and managing risk.
The challenge of supporting people with complex needs where statutory or local commissioning eligibility is not met, appears to continue across Devon.
SAR Erik
The aim of this framework is to provide a set of over-arching principles that can be utilised within all areas within the partnership footprint.
2. What is the MARM framework?
The MARM framework provides a structured and coordinated approach to support timely and effective information sharing for adults who are exhibiting high-risk behaviours or are at significant risk of harm due to their current circumstances.
It encourages a collaborative, preventative, and early intervention-focused response, aiming to reduce risk and improve outcomes for the adult’s health and wellbeing.
At its core, the MARM framework enables partner agencies to work together to support adults where a high level of risk has been identified – particularly in situations where the adult may not be known to all agencies, may not meet eligibility criteria for certain services, or where the concerns fall outside the scope of statutory safeguarding duties.
The MARM framework does not replace usual referral routes for appropriate assessment and access to services.
Representation from a cross section of partner agencies is crucial to facilitate the most appropriate solutions for an adult where high risk has been identified.
The framework promotes a dynamic approach that encourages senior management within each partner organisation to support more flexible and creative practices.
This includes ensuring access to specialist support and legal advice for practitioners when needed, enabling earlier intervention in high-risk circumstances, involving the adult, and strengthening local partnership networks and relationships.
It is acknowledged that while a preventative early intervention-focused response should be priority however, practitioners often face complex, long-standing high-risk concerns and behaviours that may also require a solution focussed approach.
This must be supported through a multi-agency framework to ensure the involvement of all relevant professionals, with an emphasis on building trust and rapport with the adult to work towards more positive and sustainable outcomes.
The MARM seeks to ensure:
- identification and timely sharing of high risk
- the adult’s involvement and engagement
- shared responsibility, decision making and accountability
- development of shared risk management plans
- improved outcomes for the adult at risk
The MARM’s dynamic approach is underpinned by key principles of good practice, which should guide all work with adults who exhibit high-risk behaviours or find themselves in high-risk situations:
To be trauma informed – understanding the underlying causes of behaviours and the impact trauma can have on a variety of life outcomes including an adult’s mental, physical, social, emotional or spiritual wellbeing.
To consider ‘lifestyle choices’– ensure that any action taken, particularly potentially punitive action such as the use of anti-social behaviour or other powers, are carefully considered to ensure that partner agencies are not exacerbating the adult’s vulnerability nor adding further pressure through the threat of prosecution or eviction.
To provide a holistic view – to ensure a holistic understanding of an adult’s risk circumstances, it is especially valuable to gather relevant information from all partner agencies, particularly those that may have had intermittent involvement, since levels of risk may have escalated over time.
3. Safeguarding Enquiry (Section 42) vs MARM framework
The MARM framework does not replace statutory safeguarding adult duties as outlined in Section 42 of the Care Act (2014). There are duties to make enquiries when Section 42 (1) of the Care Act (2014) are met:
- An adult has needs for care and support (whether or not the authority is meeting those needs).
- Is experiencing, or is at risk of, abuse or neglect.
- And as a result of those needs, is unable to protect himself or herself against the abuse or neglect, or the risk of it.
Although not formally defined in the Care Act 2014, care and support needs refers to assistance adults may require and can be a combination of practical, financial, emotional assistance required to support the adult to live well with illness, disability, or other health conditions. This includes adults affected by dementia, learning disabilities, mental health or physical health conditions.
Not all adults who find themselves in high-risk situations will be considered to have care and support needs, and not all adults in high-risk situations will be experiencing or be at risk of abuse or neglect.
The MARM framework is a non-statutory but formal multi-agency framework which supports the management of high-risk situations involving adults who may not meet the criteria for a formal safeguarding enquiry but still experience high risk, often due to self-neglect, refusal of support or due to complex needs.
The focus is on proactive, preventative action and collaborative planning ensuring a multi-agency response to reduce or manage the risk.
4. Multi-disciplinary team (MDT) meeting vs MARM framework
To support effective collaboration and decision-making, it is also important to distinguish between a MDT meeting and a MARM meeting.
A MDT meeting’s purpose is to ensure a holistic, person-centred approach to care by coordinating input from various professionals involved in an adult’s support:
- Focus: Planning and coordinating care, treatment, and support for an adult with complex needs.
- Participants: Professionals such as doctors, nurses, social workers, therapists, and other specialists.
- Example: An MDT might be held for a patient with a complex medical condition to align on treatment, rehabilitation, and ongoing care and support plan and provision.
A MARM meeting aims to address high-risk situations where there are concerns about significant harm to an adult, or others. This framework brings together partner agencies to manage and reduce risk, promoting better outcomes for the adult.
5. When to use the MARM framework
High risk behaviours or circumstances can take many forms and may lead an adult to find themselves in situations where they are considered to be at risk of significant harm.
Significant harm is ‘an event which is life threatening and/or traumatic and from which recovery, whether physical or psychological, can be expected to be difficult or impossible’.
In these circumstances, an adult may only be known by, or come to the attention of, one agency. Where it is identified that the risks or circumstances require a collaborative multi-agency approach to sharing and managing those risks, whereby partner agencies contribute to holistic risk assessment and agree the actions required, and by whom, the MARM framework should be considered.
Examples of when the MARM framework should be considered:
- Concerns of abuse or neglect which includes self-neglect behaviours (including hoarding behaviours and increased fire safety concerns) where Section 42 criteria not met (such as when the adult is considered able to protect themselves but remain at high-risk).
- Where there is high-risk and the adult is not engaging with a network of support or disengage from existing support structure.
- Domestic abuse circumstances that do not meet MARAC or Section 42 criteria.
- Mental health concerns resulting in high-risk circumstances i.e. suicide ideation.
- Substance misuse concerns resulting in vulnerability that could lead to exploitation if not addressed.
- Homelessness, which is often associated with anxiety, depression, PTSD, and other mental health conditions where the stress of survival, isolation, and trauma significantly increase the risk of chronic illnesses, infections and risk to exploitation.
- Complex needs and/or behaviours posing significant risk of harm to the adult or to others.
- Risks previously addressed via a section 42 enquiry but for which the need for on-going risk management and monitoring has been identified.
This is not an exhaustive list; however, the key priority remains the identification of high-risk situations that necessitate a coordinated, multi-agency response to effectively manage the risks and work towards improved outcomes for the adult.
An essential element of the MARM framework is a MARM meeting which facilitates the multi-agency collaboration between partner agencies.
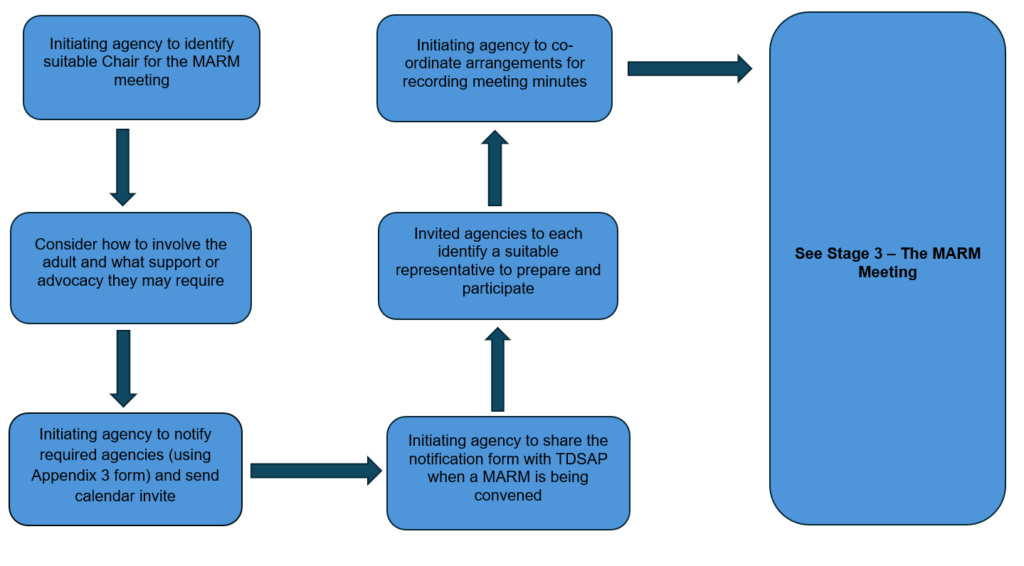
Any partner agency can initiate a MARM meeting under the framework, however, a responsible manager from that agency should be involved in the decision-making process. This agency will take the lead coordinating role with the responsibility for convening and chairing the meeting.
6. MARM framework practice principles
Prior to the introduction of a MARM process, the following principles should be applied and integrated into risk management policy and practice across all organisations:
- Partner agencies have a vital role in ensuring early interventions with adults and their representative or families, working towards preventing the deterioration of a situation or breakdown of their support network.
- Partner agencies should work collaboratively, aiming to achieve the best outcome for the adult, whilst satisfying legal, professional and organisational responsibilities and duties.
- Partner agencies should ensure early identification and assessment of risk and consideration of appropriate sharing to facilitate a multi-agency response as required.
- Partner agencies should take appropriate action within an appropriate timescale.
- The timescales adopted will be based on decisions regarding a range of factors including the risk level, complexity of the circumstances, and a consideration of the adult’s needs and wishes.
- The rights of adults and the duties, powers and responsibilities of local authorities, health, housing, police as well as other agencies remain fundamental within the MARM framework.
- Any agency can initiate a multi-agency risk management meeting. However, a responsible manager from that agency should be involved in the decision-making process.
- The process should be person-centred and designed around the adult’s needs and wishes. The adult should be encouraged to engage and participate in the management of the risks they are experiencing including attendance at MARM meetings and holistic risk assessment.
- Personalised information, advice, support and appropriate advocacy are essential components of the MARM framework and to ensure adults are empowered to make informed decisions regarding their safety.
- Consent should be sought from the adult to involve relatives, unpaid carers, or friends, etc. to ensure those close to the adult are aware of the risk as a means of building and/or strengthening the adult’s support network.
- Practitioners should adopt a flexible, innovative and solution focused approach to mitigating risk. This may involve exploring new ways of working or re-evaluating previous options.
- Each partner agency involved in a MARM process must allocate a lead representative who are able to agree actions and relevant operational decisions.
- Consideration should be given to involving partner agencies who may previously have been involved with the adult and hold essential information or may need to get involved again. Also, agencies to whom the adult may not be known but may be crucial to be involved based on the risk identified.
- It is essential when convening a MARM meeting, to ascertain the role of the agencies who may be involved with the adult as to ensure assumptions are not made regarding what other agencies may or may not be dealing with.
- The MARM plan must be proportionate and focus on the prevention, reduction, or removal of future risk of harm as far as is possible. This plan will be jointly owned by the adult and the practitioners working with them.
- Practitioners will be responsible for identifying, assessing, and recording areas of risk and actively responding to those identified risks in a collaborative way.
- All decisions and actions taken throughout the MARM process must be clearly and accurately documented. This includes recording the practitioners involved in the decision-making and the rationale behind each decision, to ensure transparency and support defensible decision-making.
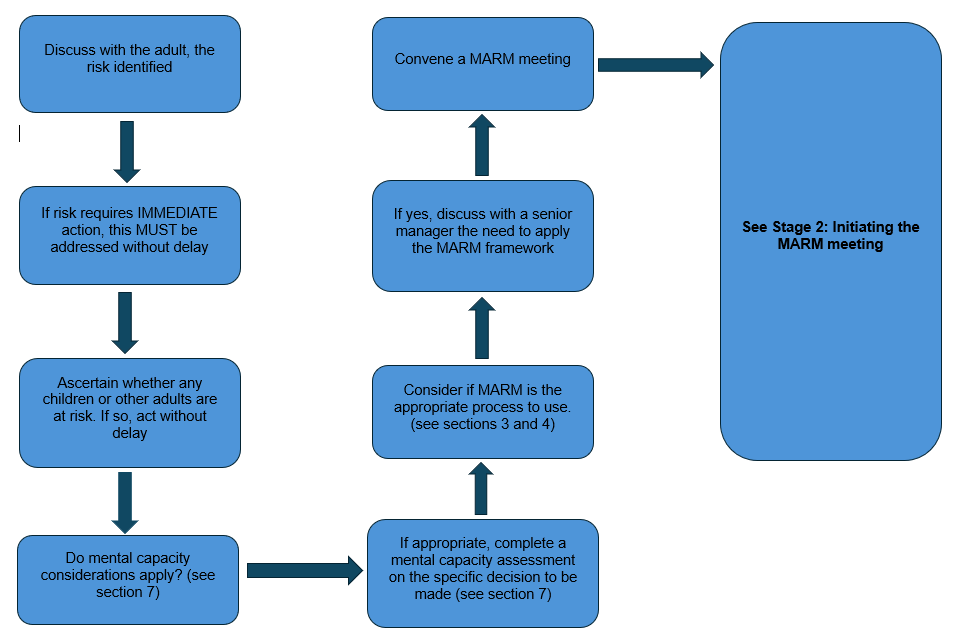
7. Mental Capacity Act (2005) and best interests
The Mental Capacity Act (2005) is designed to protect and empower people who lack the mental capacity to make their own decisions about their care and treatment. It applies to people aged 16 and over.
A person’s mental capacity, or ability to make a certain decision, may be impacted by:
- a stroke or brain injury
- a mental health problem
- dementia
- a learning disability
- confusion, drowsiness or unconsciousness because of an illness of the treatment for it
- substance misuse
The main reason for assessing mental capacity is to work out if a decision needs to be made by another person or persons.
Where there is cause to doubt a person’s ability to make a specific decision, the five principles of the Mental Capacity Act (2005) must be applied and the person’s mental capacity must be formally assessed.
In relation to the MARM framework, there may be cause to doubt an adult’s mental capacity to make decisions in circumstances such as those provided below:
- Is refusing or not co-operating with partner agencies including support services set up to provide for their health or social care needs.
- Appears to be having difficulty making necessary decisions about their health, wellbeing and safety, including decisions about the level of high risk they are experiencing.
A situation where a person is neglecting to care for themselves including not taking the necessary actions regarding the high-risk circumstances they are experiencing, and being resistant to support, likely arises from a complex personal history which may include childhood or later trauma, mental illness, acquired brain injury, abusive relationships, addiction. Rarely is self-neglect or exhibiting high risk behaviours the result of a ‘lifestyle choice’.
Any of these factors can seriously impair a person’s ability to make good decisions. Often there is an accompanying lack of trust in those in a position of authority. Carrying out a formal assessment of mental capacity with a person who is resistant or mistrustful, is very challenging.
As part of the assessment of any situation considered under this process, an opinion about the person’s ability to make key decisions – their mental capacity – needs to be formed. An assessment of mental capacity is a formalised process under the Mental Capacity Act 2005.
It is important to distinguish a decision made with mental capacity, but which others view as being ‘unwise’, from an inability to make a decision. People rarely choose to do things which are contrary to their wishes unless there is a problem with their decision-making.
This might involve not understanding the consequences of decisions. In order to think about this, we need to understand the views and wishes of the person. If a person’s actual decisions appear contrary to their known wishes this is likely to be an indication of incapacity.
The MARM meeting should include a discussion of the person’s decision making. It is important to be clear what has led to a concern about their mental capacity.
The meeting record should clearly indicate current opinions about mental capacity and detail any plan to formulate an assessment. Careful consideration is needed about who is best placed to make the assessment.
Assessments of mental capacity will need to give due consideration to the presence of executive functioning difficulties which is evident if they are unable to put a decision they have made into practice.
Assessments should draw upon a range of sources of evidence including the knowledge of their situation by others. A mental capacity assessment based solely upon a conversation with the person is likely to miss out key information.
The need for a wide range of evidence is especially important if it is difficult to engage the person in a more formal assessment interview.
When someone is believed to be lacking mental capacity to make decisions for themselves, practitioners should always consider:
- Does there need to be a formal assessment of mental capacity for any decision(s) related to the high-risk concerns raised?
- Whether the person’s lack of mental capacity might be temporary and therefore whether any decision-making can be delayed.
- The wishes, feelings, values and beliefs of the person who has been assessed as lacking mental capacity.
- The views of family members, parents, carers and other people interested in the welfare, if this is practical and appropriate, of the person who has been assessed as lacking mental capacity.
- The views of any person who holds a valid Enduring Power of Attorney or a Lasting Power of Attorney (finance and/or health and welfare) made by the person now lacking mental capacity (the register of LPAs and EPAs held by the Office of the Public Guardian can be checked on referral)
- The views of any deputy appointed by the Court of Protection to make decisions on the person’s behalf.
- Any other information that may be relevant.
8. Confidentiality and consent in high-risk information sharing
It essential to balance confidentiality with the duty to protect adults and the public. The following golden rules of information sharing provide professionals with a framework of how to approach information sharing.
Data protection legislation and human rights law are not barriers to justified information sharing.
The following legislation provides legal powers for partner agencies to share information in circumstances where the sharing is necessary to protect an adult or child from harm.
- Section 17 of the Children Act 1989 – Duty to safeguard and promote the welfare of a child.
- Section 10 of the Children Act 2004 – Duty to cooperate with partners to improve the wellbeing of a child.
- Section 11 of the Children Act 2004 – Duty to ensure services have regard for the need to safeguard and promote the welfare of children.
- Section 1 of the Care Act 2014 – Duty to promote an adult’s wellbeing
- Section 2 of the Care Act 2014 – Duty to prevent or delay an adult’s the need for care and support
- Section 3 of the Care Act 2014 – Duty to promote the integration of care and support with services to promote an adult’s welfare.
- Section 251B of the Health and Social Care Act 2012 – Duty to share information, the disclosure of which would facilitate the provision to the individual of health services or adult social care.
Provided that one of these lawful duties applies to the sharing of information, practitioners and their respective agencies will have lawful grounds to share the information.
Be open and honest with the individual and/or their family where appropriate
Ensure that as practitioners you are engaging adults who may be the subject of concerns and where appropriate their family, and or legal representative if it is safe and appropriate to do so.
Where possible individuals should be informed about how their personal data will be shared, with whom it will be shared and what effects this sharing may have on them.
Seek advice if you are not sure
If you are not sure whether you have grounds to share personal data, you should seek advice from fellow practitioners, or from your organisation’s Data Protection Officer.
Share with informed consent where appropriate
If the proposed sharing is not required to deliver a statutory duty, we should seek the consent of the adult before sharing their personal data and where possible, we should respect the wishes of those who do not consent to the sharing of their personal data.
Please remember that you may still share personal data without consent if, in your judgement, there is good reason to do so, such as where safety to the data subject or others may be at risk if you don’t share.
Consider safety and well-being
When you are considering if you can share personal data you must always consider whether the sharing is needed to keep the data subject, people who may be working with them or others safe from harm. If you are intending to share for this purpose you will have legal grounds to support the sharing.
Sharing must be necessary, proportionate, relevant, adequate, accurate, timely and secure
Ensure that any personal data you share is necessary for the purpose for which you are sharing it, is shared only with those individuals who need to have it, is accurate and up-to-date, is shared in a timely fashion, and is shared securely.
Keep a record of your decision and the reasons for it
If you decide to share information, you should keep a record of what you share and the reasons for it. This will be useful if your decisions are challenged in the future.
Engage your Caldicott Guardian
A Caldicott Guardian’s role is to oversee the sharing of information and to ensure that any sharing is lawful, fair proportional, transparent and ethical.
9. Stages of the MARM framework
Please see stages one, two, three and four of the MARM framework process below.
Stage one: High risk identified
Stage two: Initiating the MARM meeting – role of the initiating partner
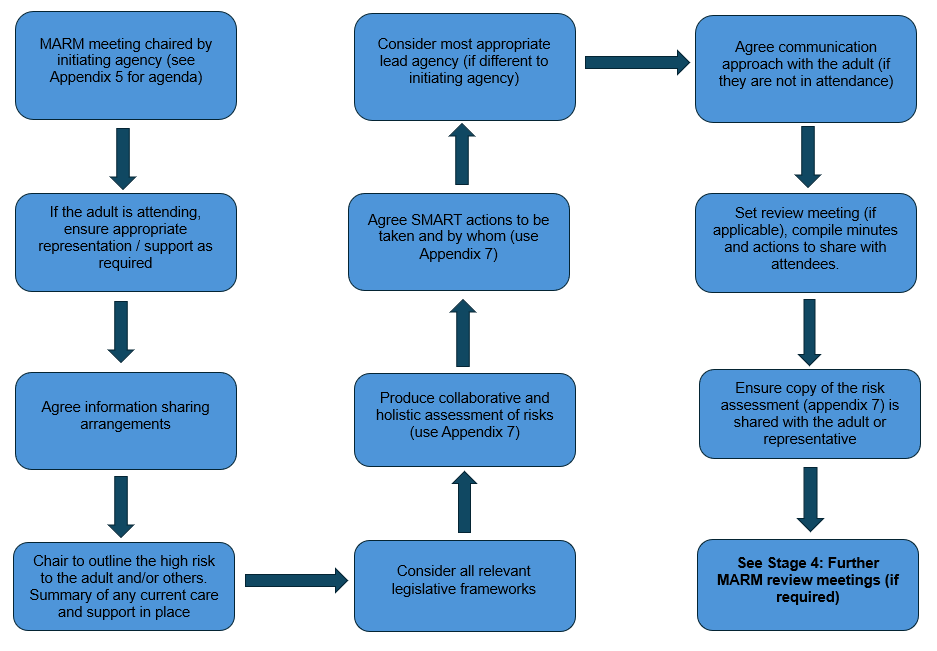
Stage three: The MARM meeting
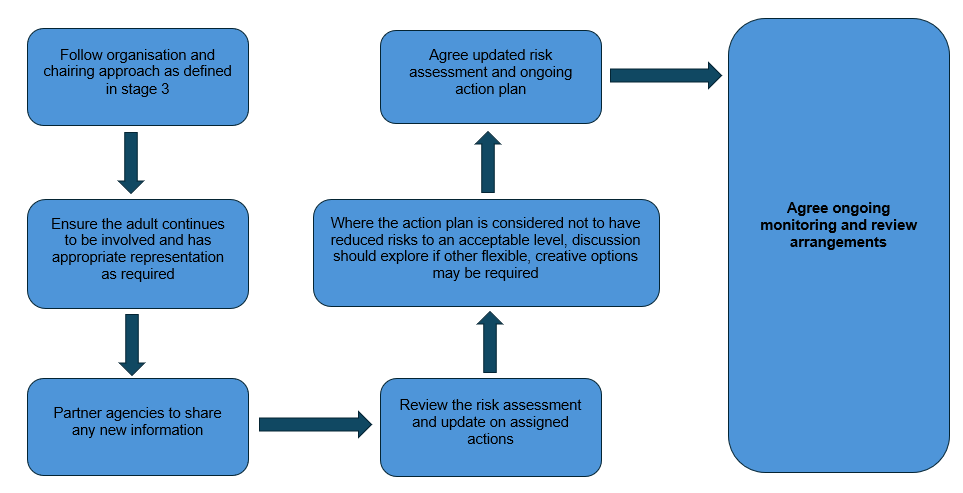
Stage four: Further review meetings (if required)
Follow up MARM review meetings can be agreed to support multi-agency monitoring and to ensure the identified high risks either resolves, is managed to an acceptable level or provides opportunity for further multi-agency collaboration despite the previously agreed action plan.
You may already know who to contact in other agencies to arrange a MARM, however we understand that you may need some support with this. We are not able to share contact details for each partner agency online, however, your agency have been provided with a list of relevant contact details from all key organisations across Torbay and Devon. Please contact your internal MARM lead for these. If you need to find out who this is, please contact the Safeguarding Adults Partnership directly by emailing safeguardingadultsboardsecure-mailbox@devon.gov.uk for assistance.
Attendees to be considered as appropriate (this is not an exhaustive list):
- Devon and Cornwall Police (DCP)
- Devon County Council (Integrated Adult Social Care – IASC)
- Torbay Council (ASC)
- Devon Partnership Trust (DPT)
- NHS Devon Integrated Care Board/Primary Care
- Royal Devon University Healthcare NHS Foundation Trust (RDUH)
- Torbay and South Devon NHS Foundation Trust (TSDFT)
- University Hospitals Plymouth NHS Trust (UHP)
- Together Drug and Alcohol Service
- South Western Ambulance Service NHS Foundation Trust (SWAST)
- Torbay Community Safety Partnership
- Safer Devon Partnership
- Devon and Somerset Fire and Rescue Service
- The Probation Service – Devon and Torbay
For district council involvement:
- East Devon District Council
- Exeter City Council
- Mid Devon District Council
- North Devon District Council
- South Hams District Council
- Teignbridge District Council
- Torridge District Council
- West Devon Borough Council
You can contact voluntary sector organisations directly to confirm where the MARM notification form and invite should be sent.
Should you have any difficulties ascertaining the most appropriate contact person in housing providers or voluntary sector partners, please contact the TDSAP mailbox for support safeguardingadultsboardsecure-mailbox@devon.gov.uk.
Governance and oversight
The partnership will provide strategic oversight of the MARM framework. To support this, TDSAP will be notified when a meeting is being convened under the MARM framework.
Any learning themes identified will form part of future guidance and practice development.
Each partner agency has a designated MARM champion and deputy. The role of the champion is specifically to ensure awareness and act as a point of escalation should support be required at a strategic level for example engagement and attendance.
The route for accessing the MARM champion for a specific partner agency is by contacting the TDSAP mailbox at safeguardingadultsboardsecure-mailbox@devon.gov.uk.
Appendix one: The ‘case for change’
SAR Erik
The Torbay and Devon Safeguarding Adults Partnership (TDSAP) commissioned a safeguarding adults review (SAR) around the death of Erik, aged 48, who was found hanging from scaffolding in Exeter on 1 April 2021.
Erik has been described as having had very poor social skills with mild/moderate learning disabilities.
There have been several significant tragic events in Erik’s life that may have contributed to a lifestyle or certain behaviour. Devon and Cornwall Police identified that Erik was a victim of ‘cuckooing’ for some time before and at the time of his death.
Further research into Erik as a victim of cuckooing identified that this form of exploitation had been a factor in his life since 2013.
The National County Lines Coordination Centre has identified a number of specific heightened risk factors that make people vulnerable to cuckooing. Many of these directly relate to Erik:
- Lack of safe or stable home environment.
- Social isolation or social difficulties.
- Economic deprivation.
- Insecure accommodation status.
- Physical or learning disability.
- Mental ill health.
- Substance misuse.
The response to cuckooing cannot be reliant on a single agency, nor law enforcement. This is particularly so when the legislative framework is limited. A multi-agency response to adult victims of exploitation needs to be supported by clear guidance for practitioners bringing together the various powers, skills and funding streams in a collaborative and person centric approach.
Both police officers and housing officers attempted to safeguard Erik. There are examples of good proactive action such as installing a dummy alarm, regular visits to Erik’s address, referrals to other agencies. It is clear that police officers and housing officers did work together.
However, it is recognised that a multi-agency risk management framework would have supported a collaborative approach to sharing the high risk and facilitated a co-ordinated action plan at the earliest opportunity. Safeguarding concern referrals were raised however the response to this was delayed and impacted on by the pandemic.
The MARM framework was developed following statutory review recommendations which highlighted that a collaborative, preventative approach of sharing risk and actions between partner agencies are crucial to achieve better outcomes for adults.
The recommendations from SAR Erik that are pertinent to this framework are:
Within six months, The TDSAP together with Safer Devon Partnership, Devon Children and Families Partnership and The Devon Anti-Slavery Partnership, consider how best to develop a multi-agency framework to enable practitioners to minimise the risk of adult victims of cuckooing being exploited.
This framework to include data collection, potential powers that can be employed to disrupt or prosecute perpetrators, support available to victims, raising community awareness of exploitation and learning opportunities for practitioners (the National County Lines Coordinating Centre is a potential source of valuable information for developing such a framework including national training packages).
The TDSAP at its December 2022 Board meeting accepts the following three-part recommendation:
- By 31 December 2022, the TDSAP instigates a task and finish group to clearly understand the need for a multi-agency risk management process to safeguard people with complex needs who do not meet eligibility criteria for statutory or local commissioning support. This initial phase of work to include what currently exists across the Devon County Council footprint, and examples of similar work across the UK.
- By 31 March 2023, the task and finish group provides the TDSAP with options as to how this cohort of people can best be safeguarded across Devon.
- By 31 December 2023, TDSAP is implementing its preferred option with tangible improvement in safeguarding outcomes for people with complex needs who are not within statutory or local commissioning processes.
SAR Rita
Rita was 49 years old when she died at the Royal Devon and Exeter Hospital (RD&E) on 20 October 2017. She had been admitted to the hospital on 14 October 2017 following a 111 call by her partner as he was concerned about her apparent breathing difficulties. She did not recover consciousness.
The initial safeguarding referral from the RD&E outlined significant concerns about her physical condition, a significant number of what appeared to be burn marks on her body and known use of crack cocaine and IV drug use. At the inquest hearing on 14 August 2018 the following findings and determinations were made: The medical cause of death was infective endocarditis and intravenous drug use.
Rita had a diagnosed learning disability and was known to several agencies. Agencies use different recording systems which can inhibit information sharing and communication.
It was felt that to communicate, understand and respond appropriately to risk for vulnerable adults with support needs, there needs to be a coordinated and collaborative response to sharing information. This could have facilitated a multi-agency risk management meeting with a preventative approach.
Rita’s property was described by professionals as basic and sparse. The property was observed to be mouldy in 2014. The Primary Care Liaison Nurse reported that in 2016/17 furniture was blood stained due to wounds on Rita’s body caused by IV drug use.
It was housing staff who first raised concerns about Rita in April 2013. It may well have been the right decision at this time for a social care assessment to be undertaken as a proportionate response to the risk and due to the differing views in terms of the level of self-neglect.
It is possible that housing staff felt unable to challenge the decision made at this time not to take further action under Section 42(1) safeguarding enquiry criteria.
In October 2015, Rita’s safeguarding social worker made a referral to the Intensive Assessment and Treatment Team (IAAT). IAAT did not accept the referral as their criteria was not met but this was not fed back to the Safeguarding Team.
If a referral is made between agencies and teams and this referral is not accepted, then it is essential that this is fed back to the referrer and steps are in place for the referring team to review their decision making. This emphasises the importance of partner agencies and professionals having an understanding of other organisations’ roles and referral criteria.
Professionals reflecting at the learning event agreed that the 2nd safeguarding referral in October 2015 should have met the criteria for a Section 42 safeguarding enquiry. Had Rita been discussed within a multi-agency forum this decision may have been taken at the time.
There is no evidence available to suggest that staff considered that Rita’s ability to make capacitated decisions regarding her life choices and health decisions might have fluctuated.
There are many factors that could lead to Rita’s capacitated decision-making being compromised, including but not limited to; her variable emotional or mental health, poor physical health and infections, her difficulties associated with drugs and alcohol, as well as external pressures or influences.
If there is reason to be concerned that an adult’s mental capacity for a specific decision may be affected as is indicated in Rita’s case, staff need to ensure that consideration of this is recorded, and assessment outcomes are clearly evidenced.
The recommendations of SAR Rita that are pertinent to this framework are:
Whole system acknowledgement that when working with people with complex needs whom professionals, services and agencies find difficult to support; there needs to be joined up support and planning which ensures the most effective engagement to the persons unique circumstances.
There needs to be clarification and development of consistent terms of reference for forums across the health and social care system and the county, for example, Core Groups need to be used in a consistent way across the county and include all adults of concern regardless of age.
A multi-agency risk management forum should be put in place in Devon to consider cases of complexity and risk such as self-neglect and other high-risk situations, where staff are struggling with how to manage or reduce the risk.
To support practitioners, a multi-agency risk management forum would require senior level representation and offer a fresh approach with creative solutions, access to specialist support and legal advice where appropriate.
Appendix two: MARM overview flowchart
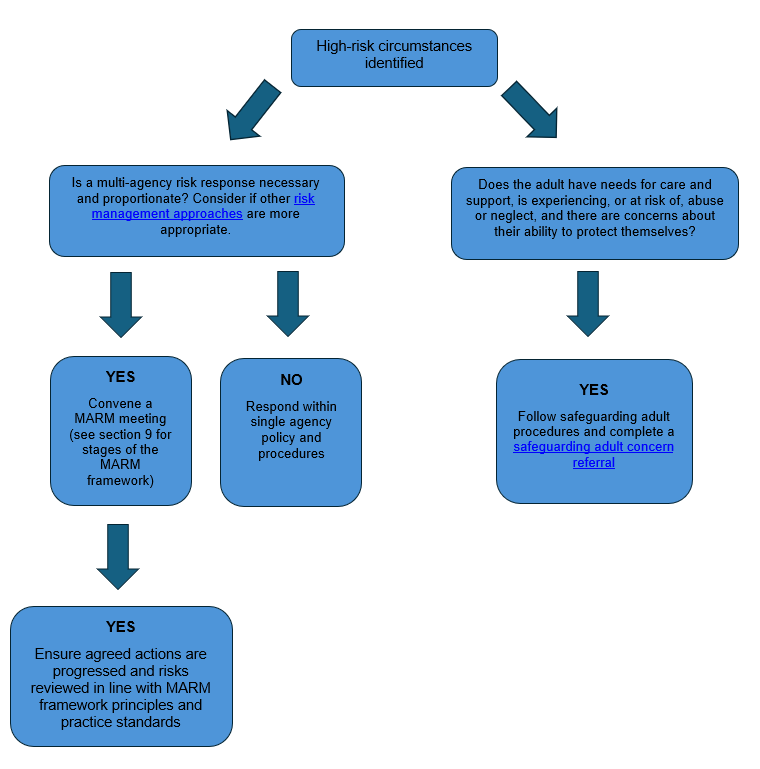
Links included in the flowchart:
Appendix three: MARM meeting notification form
Download a MARM meeting notification template
Appendix four: Guidance on chairing MARM meetings
Introduction
Any meetings convened under the MARM framework should be chaired by someone who, as a minimum requirement, is a senior member of staff (for example, local authority senior practitioner, Band 7 nurse, substantive police sergeant, registered care home manager, voluntary organisation manager or equivalent).
Preparing for the meeting
At the outset of initiating the MARM framework, a discussion should take place with the adult about whom high risk behaviours or circumstances have been identified to establish if they wish to attend any of the meetings.
There may be situations where an adult may not want to attend, may not be able to attend (for example due to mental capacity), or exceptionally, where it may not be appropriate for them to attend. Consideration should be given to holding the meeting in a neutral space, for example, GP surgery, ward, and somewhere close to where the adult lives.
Prior to the meeting, the practitioner working with the adult should meet with them to help prepare them to attend; this may include the involvement of their representative as necessary.
This should include the following:
- The purpose of the meeting, what it will cover and its confidential nature.
- Whether the adult has any communication or access needs.
- Confirm who the attendees to the meeting will be and the agencies they represent.
- Whether the adult will attend the whole meeting or part of the meeting, for example, if police intelligence is being shared it may not be appropriate for the adult to attend during that part.
- Confirm the adult’s views and wishes and what they would wish the outcomes of the meeting to be.
The meeting
- Meeting chaired by a senior member of staff from the initiating agency (as described above).
- Ensure the adult has appropriate representation or support as required.
- Welcome attendees to the meeting and request they introduce themselves including their role and the partner agency they represent. Request that electronic devices are set to silent and confirm that they are able to remain for the whole meeting.
- Ask professionals not to use jargon and advise the person with care and support needs that they can ask for things to be re-phrased or repeated if they do not understand.
- Agree information sharing arrangements at the start.
- Outline the high risk to the adult and/or others that has been identified.
- Confirm the adult’s expressed views and wishes.
- Provide a summary of any care and support currently in place.
- Consideration of all relevant legislative frameworks.
- Produce a collaborative and holistic assessment of the risks identified, which must reflect the adult’s views and wishes, and develop SMART actions to be taken with timescales a named lead against each action.
- Consider which agency is most appropriate to be the lead agency or whether this remains the initiating agency.
- If the adult is not in attendance, consider how communication will take place with the adult and how they will be kept informed and by whom.
- Set a date for a review meeting and agree what specific high-risk indicators may trigger a more imminent review meeting.
- Ensure the adult is given a copy of the risk assessment and agreed actions.
In complex circumstances where the risk remains significantly high, the nature and frequency of review meetings will vary.
The minutes of the meetings should be succinct and contain clear information regarding the discussion points and will be circulated to attendees marked ‘Strictly confidential‘.
Appendix five: MARM meeting agenda template
Download a template for use when creating a MARM meeting agenda
Appendix six: MARM meeting minutes template
Download a template for use when taking MARM meeting minutes
Appendix seven: MARM risk assessment tool
Download the MARM risk assessment tool