Contents
Introduction
This guidance confirms the commitment of all members of the Torbay and Devon Safeguarding Adults Partnership to keeping safe the adults at risk with whom member organisations works alongside or who live in the geographical boundaries of Torbay County Council and Devon County Council. Members of the Torbay and Devon Safeguarding Adults Partnership acknowledge their duty to act appropriately to any allegations, reports or suspicions of abuse.
The Torbay and Devon Safeguarding Adults Partnership believes that it is important to have both guidance and procedures in place so that all managers, staff, volunteers, service users and carers can work together to prevent abuse and know what to do should a concern arise.
Purpose and how to use this document
The purpose of this document is to better safeguard adults at risk of abuse throughout Torbay and Devon; and in using this document better encourage the continuous development of best practice. It covers the legislative requirements and expectations on individual services to safeguard and promote the well-being of adults in the exercise of their respective functions, relating to adults with needs for care and support and carers; and a framework for the TDSAP to monitor the effective implementation of policies and procedures.
The document is structured into the following sections and appendices:
Section 1: Context, Principle and Values sets out the shared vision for adult safeguarding and the key national and local drivers
Section 2: Adult Safeguarding Guidance sets out an interpretation of the Care Act 2014, so that there is a consistent approach across Torbay and Devon to adult safeguarding.
Section 3: Adult Safeguarding Practice includes the key areas of mental capacity and consent, advocacy and support, managing risk, record keeping and organisational learning.
Section 4: Adult Safeguarding Procedures sets out the changes in adult safeguarding from a process driven stand-alone entity, to one where adult safeguarding is part of everyday practice about supporting adults who are unable to protect themselves without support towards achieving better outcomes for their safety and well-being. It provides the reader with a framework that can be adjusted to meet individual need.
Appendix 1: Details the structures and organisations who work with adults at risk. It provides detail on the TDSAP roles and responsibilities and the links to other strategic partnerships. It sets out the changes brought about by the Care Act 2014 for the role and responsibilities of the statutory organisations and lists those organisations who work together to safeguard adults at risk.
This document should be read in conjunction with the following documents:
This document embeds relevant national developments and draws on the commitment for organisations to work together as championed by the Association of Directors of Adult Social Services.
It is steered by the personalisation of health and adult social care through the national Making Safeguarding Personal programme. This programme arose following feedback from many people who had used safeguarding services, reporting that they felt they were being driven through a process and felt out of control. The shift in culture, by developing a personalised approach to supporting people is a shared vision for all organisations working with adults who may be or are at risk of abuse and neglect.
The Mental Capacity Act 2005 is relevant throughout safeguarding practice, and staff should ensure that all decisions and actions are taken in line with the requirements of the Act.
Reference to key resources are made throughout in particular:
Section 1: Context, principles and values
1.1 Context
The Care Act (2014) puts adult safeguarding on a legal footing and requires each Local Authority to set up a SAB, within Torbay and Devon this is referred to as TDSAP, with core membership from the Local Authority, the Police and the NHS (specifically local Clinical Commissioning Group/s). It has the power to include other relevant bodies. Each organisation involved in adult safeguarding also has obligations under data protection legislation. One of the key functions of the TDSAP is to ensure that the policies and procedures governing adult safeguarding are fit for purpose and can be translated into effective adult safeguarding practice.
TDSAP have revised their multi-agency safeguarding adult’s guidance and procedures so that there is consistency across Torbay and Devon in the way in which adults are safeguarded from neglect or abuse, and in how information is shared for that purpose. All organisations involved in safeguarding are asked to adopt this revised guidance and procedures in respect of their relevant roles and functions, but may wish to add local practice guidance, protocols and organisation operation manuals.
1.2 Principles
The guidance and procedures are based on the Six Principles of Safeguarding that underpin all adult safeguarding work:
Empowerment
Adults are encouraged to make their own decisions and are provided with support and information.
I am consulted about the outcomes I want from the safeguarding process and these directly inform what happens
Prevention
Strategies are developed to prevent abuse and neglect that promotes resilience and self-determination.
I am provided with easily understood information about what abuse is, how to recognise the signs and what I can do to seek help.
Proportionate
A proportionate and least intrusive response is made balanced with the level of risk.
I am confident that the professionals will work in my interest and only get involved as much as needed.
Protection
Adults are offered ways to protect themselves, and there is a co-ordinated response to adult safeguarding.
I am provided with help and support to report abuse. I am supported to take part in the safeguarding process to the extent to which I want and to which I am able
Partnerships
Local solutions through services working together within their communities.
I am confident that agencies will work together to find the most effective responses for my own situation
Accountable
Accountability and transparency in delivering a safeguarding response.
I am clear about the roles and responsibilities of all those involved in the solution to the problem
The Care Act (2014) and care and support stautory guidance states that safeguarding:
- is person led
- engages the person from the start, throughout and at the end to address their needs
- is outcome focused
- is based upon a community approach from all partners and providers
This TDSAP multi-agency safeguarding adult’s guidance is built on strong multi-agency partnerships working together with adults to prevent abuse and neglect where possible and provide a consistent approach when responding to safeguarding concerns.This entails joint accountability for the management of risk, timely information sharing, co-operation and a collegiate approach that respects boundaries and confidentiality within legal frameworks.
1.2.1 Risk management
Safeguarding is fundamentally about promoting the safety and well-being of an adult in line with the above six principles. This involves risk management, which is used:
- to promote, and thereby support, inclusive decision making as a collaborative and empowering process, which takes full account of the individual’s perspective and views of primary carers
- to enable and support the positive management of risks where this is fully endorsed by the multi-agency partners as having positive outcomes
- to promote the adoption by all staff of ‘defensible decisions’ rather than ‘defensive actions’
Effective risk management strategies identify risks and provide an action or means of mitigation against each identified risk and have a mechanism in place for early escalation if the mitigation is no longer viable. Contingency arrangements should always be part of risk management. Risk assessments and risk management should take a holistic approach and partners should ensure that they have the systems in place that enable early identification and assessment of risk through timely information sharing and targeted multi-agency intervention (See practice section 3).
Where an individual is not able to protect themselves without support, the aim should be to support them to make their own informed decisions which preserve their safety. However, people involved in safeguarding need to acknowledge that there is a balance to be struck between risk and an individual’s right to make their own informed decisions, even if others consider the decision to be unwise or puts the individual at risk. The importance of their right to make decisions about their own life, which is part of an individual’s well-being, needs to be considered as well as the safeguarding concerns.
1.2.2 Co-operation
The local authority holds the statutory duty in relation to safeguarding adults and is responsible for the public law decision as to whether or not to proceed to the duty to make safeguarding enquires under section 42(2). Local authorities and partner organisations should co-operate in order to deliver effective safeguarding, both at a strategic level and in individual cases, where they may need to ask one another to take specific action in that case. This co-operation and information sharing for safeguarding purposes is supported by all data protection legislation where there is a lawful basis, such as the Care Act, for sharing personal data and compliance with the caldicott principles will help to ensure that information sharing is justified and proportionate.
Section 6, the Care Act 2014 describes a general duty to co-operate between the local authority and other organisations providing care and support. This includes a duty on the local authority itself to ensure co-operation between its adult care and support, housing, public health and children’s services.
Local authorities and their relevant partners must respond to requests to cooperate under their general public law duties to act reasonably.
If an organisation is refusing to share information, the organisation conducting an enquiry can escalate to TDSAP to consider using section 5, Care Act 2014 powers, which puts an obligation on organisations to comply with a request for information in order that the TDSAP can perform its duties.
The Care Act 2014 sets out five aims of co-operation between partners which are relevant to care and support, although it should be noted that the purposes of cooperation are not limited to these matters. The five aims include:
- promoting the wellbeing of adults needing care and support and of carers
- improving the quality of care and support for adults and support for carers (including the outcomes from such provision)
- smoothing the transition from children to adults’ services
- protecting adults with care and support needs who are currently experiencing or at risk of abuse or neglect
- identifying lessons to be learned from cases where adults with needs for care and support have experienced serious abuse or neglect.
Organisations that refuse to comply with requests for co-operation or information should provide written reasons for the refusal.
1.2.3 Information sharing
Sharing the right information, at the right time with the right people, is fundamental to good safeguarding practice. Section 45 of the Care Act 2014 creates a legal duty to comply with requests for information from SABs as detailed above. Sharing information between organisations as part of day-to-day safeguarding practice is governed by the Common Law Duty of Confidentiality, the Crime and Disorder Act 1998, Data Protection Act 2018, the Human Rights Act 1998, and the UK General Data Protection Regulation.
As a general principle people must assume it is their responsibility to raise a safeguarding concern if they believe an adult at risk is suffering or likely to suffer abuse or neglect, and/or are a risk to themselves or another, rather than assume someone else will do so. They should share the information with the local authority and/or the police if they believe or suspect that a crime has been committed or that the individual is immediately at risk.
Helpful guidance to ensure that information sharing is justified and proportionate is set out in the Caldicott principles. Partner organisations may be asked to share information through agreed information sharing protocols. TDSAP has a protocol in place for information sharing, with clear governance on how it will be implemented (currently being updated).
1.2.4 Confidentiality
A duty of confidence arises when information is provided by someone under circumstances where it is reasonable for them to expect that the information will be held in confidence.
Adults at risk provide sensitive information and have a right to expect that the information about themselves that they directly provide, and information obtained from others will be treated respectfully and that their privacy will be maintained.
The challenges of working within the boundaries of confidentiality should not impede taking appropriate action. Whenever possible, informed consent to the sharing of information should be obtained. However:
- emergency or life-threatening situations may warrant the sharing of relevant information with the relevant emergency services without consent
- the law does not prevent the sharing of sensitive, personal data within organisations.
- if the information is confidential, but sharing is necessary to help safeguard someone from harm, sharing it will be justified provided that the information that is shared is proportional and limited to what is necessary
- the law does not prevent the sharing of sensitive personal data between organisations, provided that the sharing is lawful and is consistent with information sharing guidance issued by the Information Commissioner’s Office (ICO).
Whether information is shared with or without the adult at risk’s consent, the information sharing process must abide by the principles of the UK General Data Protection Regulation (UK GDPR). The UK GDPR should not be a barrier to sharing information. It provides a framework to ensure that personal information about living persons is shared appropriately. SCIE has also produced helpful practice guidance in relation to information sharing with or without consent.
In those instances where the person lacks the mental capacity to give informed consent, staff should always bear in mind the requirements of the Mental Capacity Act 2005, and whether sharing it will be in the person’s best interest.
1.2.5 Well-being
Section 1 of the Care Act (2014) states that local authorities must promote wellbeing when carrying out any of their care and support functions in respect of a person. This may sometimes be referred to as ‘the wellbeing principle’ because it is a guiding principle that puts wellbeing at the heart of care and support. For safeguarding, this would include safeguarding activities in the widest community sense and is not confined to safeguarding enquiries under Section 42 of the Care Act (2014). The wellbeing principle should apply to all agencies involved in safeguarding adults.
‘Well-being’ is a broad concept, and it is described as relating to the following areas:
- personal dignity (including treatment of the individual with respect)
- physical and mental health and emotional wellbeing
- protection from abuse and neglect
- control by the individual over day-to-day life (including over care and support provided and the way it is provided)
- participation in work, education, training or recreation
- social and economic wellbeing
- domestic, family and personal
- suitability of accommodation
- the individual’s contribution to society.
Paragraphs 14.14 and 14.15 of the Care and Support statutory guidance emphasises the need for the safeguarding enquiry to be person led and outcome focused.
“14.14. In addition to these principles, it is also important that all safeguarding partners take a broad community approach to establishing safeguarding arrangements. It is vital that all organisations recognise that adult safeguarding arrangements are there to protect individuals. We all have different preferences, histories, circumstances and lifestyles, so it is unhelpful to prescribe a process that must be followed whenever a concern is raised; and the case study below helps illustrate this.
14.15. Making safeguarding personal means it should be person-led and outcome-focused. It engages the person in a conversation about how best to respond to their safeguarding situation in a way that enhances involvement, choice and control as well as improving quality of life, wellbeing and safety.”
All organisations working with adults who are or may be at risk of abuse and neglect, must aim to ensure that they are supporting people to make their own informed and safe decisions as well as taking or prompting action to protect people who are not able to protect themselves. This should underpin every activity through consistent safeguarding adults’ work. This includes any safeguarding activity that is outside the scope of a Section 42 Care Act 2014 enquiry.
1.3 Values – supporting adults at risk of abuse and neglect
Safeguarding has the highest priority across all organisations. There is a shared value of placing safeguarding within the highest of corporate priorities. Organisations are judged on the effectiveness of safe communities and their values towards safeguarding adults who may be at risk of abuse or neglect. Values include:
- people are able to access support and protection to live independently and have control over their lives
- appropriate safeguarding options should be discussed with the adult at risk according to their wishes and preferences
- they should take proper account of any additional factors associated with the individual’s disability, age, gender, sexual orientation, ‘race’, religion, culture or lifestyle
- the adult at risk should be the primary focus of decision making, determining what safeguards they want in place and provided with options so that they maintain choice and control
- all action should begin with the assumption that the adult at risk is best placed to judge their own situation and knows best the outcomes, goals and wellbeing they want to achieve
- the individual’s views, wishes, feelings and beliefs should be paramount and are critical to a personalised way of working with them
- there is a presumption that adults have mental capacity to make informed decisions about their lives.
- if someone has been assessed as not having mental capacity, to make decisions about their safety, decision making will be made in their best interests as set out in the Mental Capacity Act 2005 and Mental Capacity Act Code of Practice
- people will have access to supported decision making
- all decisions should be made with the adult at risk and promote their wellbeing and be reasonable, justified, proportionate and ethical
- timeliness should be determined by the personal circumstances of the adult at risk
- every effort should be made to ensure that adults at risk are afforded appropriate protection under the law and have full access to the criminal justice system when a crime has been committed.
Section 2:Adult safeguarding guidance
2.1 What is safeguarding?
Safeguarding is defined as ‘protecting an adult’s right to live in safety, free from abuse and neglect.’ (Care and support statutory guidance, chapter 14). Adult safeguarding is about preventing and responding to concerns of abuse, harm or neglect of adults. Staff should work together in partnership with adults so that they are:
- safe and able to protect themselves from abuse and neglect
- treated fairly and with dignity and respect
- protected when they need to be
- able easily to get the support, protection and services that they need
The aims of adult safeguarding are to:
- stop abuse or neglect wherever possible
- prevent harm and reduce the risk of abuse or neglect to adults with care and support needs
- safeguard adults in a way that supports them in making informed choices and having control about how they want to live
- promote an approach that concentrates on improving life for the adults concerned
- raise public awareness so that communities as a whole, alongside professionals, play their part in preventing, identifying and responding to abuse and neglect
- provide information and support in accessible ways to help adults understand the different types of abuse, how to stay safe and what to do to raise a concern about the safety or well-being of an adult
- address what has caused the abuse
2.1.2 Prevention
Section 2 of the Care Act requires local authorities to ensure the provision of preventative services (i.e. services which help prevent or delay the development of care and support needs or reduce care and support needs). Organisations should take a broad community approach to establishing safeguarding arrangements, working together on prevention strategies.
Prevention strategies might include:
- identifying adults at risk of abuse
- public awareness
- information, advice and advocacy
- inter-agency cooperation
- training and education
- integrated policies and procedures
- integrated quality and safeguarding strategies
- community links and community support
- regulation and legislation
- proactive approach to prevent.
Partners should embrace strategies that support action before harm can occur. Where abuse or neglect has occurred, steps should be taken to prevent it from reoccurring wherever possible, doing so within relevant parameters and sharing information in ways which are proportionate and lawful to support a holistic partnership approach to prevention. For example, visiting staff might identify an adult with a combination of characteristics that may render them more vulnerable to a fire risk and take action to refer to the Devon and Cornwall Fire Brigade for a fire safety visit.
Organisations should implement robust risk management processes that identify adults at risk of abuse or neglect and take timely appropriate action. Safeguarding functions should be integrated into quality management and assurance structures.
Prevention should be discussed at every stage of safeguarding and is especially important at the closure stage (which can happen at any time) when working with adults on resilience and recovery. Discussions between staff and adults, their personal network and the wider community (if appropriate) help build resilience as part of the recovery process. Where support is needed to prevent abuse, this needs to be identified and put into safeguarding planning.
2.1.3 Raising awareness
Public awareness campaigns can make a significant contribution to the prevention of abuse. They are more effective if backed up by information and advice about where to get help, and there is effective training for staff and services to respond. Joint initiatives to raise awareness can be very effective.
2.1.4 Information
The term ‘information’ means the communication of knowledge and facts regarding care. ‘Advice’ means helping a person to identify choices and/or providing an opinion or recommendation regarding a course of action in relation to care and support. Local authorities are required to establish and maintain an information and advice service relating to all local residents within its area, not just adults with care and support needs.
Information and advice are critical to preventing or delaying the need for services and, in relation to safeguarding, can be the first step to responding to a concern. Section 4, the Care Act states that Local Authorities must: ‘establish and maintain a service for providing people in its area with information and advice relating to care and support for adults and support for carers.’ This includes information and advice about safeguarding and should include:
- how to raise concerns about the safety or wellbeing of an adult who has needs for care and support needs
- awareness of different types of abuse (including neglect) and harm and indicators to look out for
- how people can keep safe, and how to support people to keep safe
- the safeguarding adults process
- how SABs work.
All organisations should ensure that they are able to provide this service and can signpost adults to receive the right kind of help by the right organisation.
2.1.5 Advice
Information and advice need to be tailored to the person seeking them, recognising people may need different mediums through which to communicate. Information and advice should, where possible, be provided in the manner preferred by the person and in a way to help them understand the information being conveyed. This should be carried out with an awareness of the Equality Act 2010. ‘Reasonable adjustments’ should be made to ensure that disabled people have equal access to information and advice services. Reasonable adjustments could include the provision of information in accessible formats or with communication support.
Organisations have a number of direct opportunities to provide, or signpost people to information and advice, in particular if an adult at risk (or a person who knows and cares about them) indicates or tells you that they are concerned for their safety/wellbeing:
- at first point of contact
- during or following an adult safeguarding enquiry
- safeguarding planning
- risk management
- through complaints and feedback about a service which identifies a safeguarding concern.
2.2 Who do adult safeguarding duties apply to?
In the context of the legislation, specific adult safeguarding duties apply to any adult who:
- has needs for care and support (whether or not the Local Authority is meeting any of those needs)
- is experiencing, or is at risk of, abuse or neglect
- as a result of those care and support needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect
Within the scope of this definition are:
- all adults who meet the above criteria regardless of their mental capacity to make decisions about their own safety or other decisions relating to safeguarding processes and activities
- adults who manage their own care and support through personal or health budgets
- adults whose needs for care and support have not been assessed as eligible or which have been assessed as below the level of eligibility for support
- adults who fund their own care and support
- children and young people in specific circumstances as detailed below
Outside of scope of this guidance and procedures:
Adults in custodial settings i.e. prisons and approved premises. Prison governors and National Offender Management Services have responsibility for these arrangements. The SAB does however have a duty to assist prison governors on adult safeguarding matters. Local Authorities are required to assess for care and support needs of prisoners which take account of their wellbeing. Equally NHS England has a responsibility to commission health services delivered through offender health teams which contributes towards safeguarding offenders.
2.2.1 Children and young people
The Children Act 1989 provides the legislative framework for agencies to take decisions on behalf of children and to take action to protect them from abuse and neglect. Young people who receive leaving or after care support from children and family services, are included in the scope of adult safeguarding, but close liaison with children and family service providers is key to establishing who is the best person to lead or support young people through adult safeguarding processes.
Section 11 of the Children Act 2004 places duties on a range of organisations and individuals to ensure their functions, and any services that they contract out to others, are discharged having regard to the need to safeguard and promote the welfare of children.
In all adult safeguarding work, staff working with the person at risk should establish whether there are children in the family and whether checks should be made on children and young people who are part of the same household, irrespective of whether they are dependent on care either from the adult at risk, or the person alleged to have caused harm.
Children and young people may be at greater risk of harm or be in need of additional help in families where adults have mental health problems, misuse substances or alcohol, are in a violent relationship, have complex needs or have learning difficulties.’ For further information see working together to safeguard children.
Abuse within families reflects a diverse range of relationships and power dynamics, which may affect the causes and impact of abuse. These can challenge professionals to work across multi-disciplinary boundaries in order to protect all those at risk. In particular staff may be assisted by using Domestic Abuse risk management tools such as the SafeLives Dash risk checklist. Staff providing services to adults, children and families should have appropriate training whereby they are able to identify risks and abuse to children and adults at risk. The Domestic Abuse Act 2021 aims to strengthen the support for victims of abuse by statutory agencies.
2.2.2 Transition
Together the Children and Families Act 2014 and the Care Act 2014, create a new comprehensive legislative framework for transition, when a child turns 18 (MCA applies once a person turns 16). The duties in both Acts are on the local authority, but this does not exclude the need for all organisations to work together to ensure that the safeguarding adult’s guidance and procedures work in conjunction with those for children and young people.
There should be robust joint working arrangements between children’s and adults’ services for young people who meet the criteria set out in ‘who do adult safeguarding duties apply to’ section of this document. The care needs of the young person should be at the forefront of any support planning and requires a co-ordinated multi-agency approach. Assessments of care needs should include issues of safeguarding and risk. Care planning needs to ensure that the young adult’s safety is not put at risk through delays in providing the services they need to maintain their independence, wellbeing and choice.
Where there are on-going safeguarding issues for a young person and it is anticipated that on reaching 18 years of age, they are likely to require adult safeguarding, safeguarding arrangements should be discussed as part of transition support planning and protection. Conference Chairs and Independent Reviewing Officers, if involved, should seek assurance that there has been appropriate consultation with the young person by adult social care and invite them to any relevant conference or review. Clarification should be sought on:
- what information and advice the young person has received about adult safeguarding?
- the need for advocacy and support
- whether a mental capacity assessment is needed and who will undertake it
- if best Interest decisions need to be made
- whether any application needs to be made to the court of protection
If the young person is not subject to a plan, it may be prudent to hold a professionals meeting.
2.2.3 Children and young people who abuse
If a child or children is/are causing harm to an adult covered by the adult safeguarding procedures, action should be taken under these procedures, and a referral and close liaison with children’s services should take place.
Physical and sexual abuse towards parents and other relatives (for example, grandparents, aunts, uncles) some of whom, may be adults at risk, can be carried out by adults and by young people and children, some of which can cause serious harm or death. The UK prevalence study of elder abuse identified younger adults (rather than the person’s partner) as the main perpetrators of financial abuse.
2.2.4 Young carers
In respect of young carers, Section 1 of the Care Act 2014, alongside section 96 and section 97 of the Children and Families Act 2014, offers a joined up legal framework to identify young carers and parent carers and their support needs. Both acts have a strong emphasis on outcomes and wellbeing.
2.2.5 Carers and safeguarding
Circumstances in which a carer could be involved in a situation that may require a safeguarding response includes when:
- a carer may witness or speak up about abuse or neglect
- a carer may experience intentional or unintentional harm from the adult they are trying to support or from professionals and organisations they are in contact with
- a carer may unintentionally or intentionally harm or neglect the adult they support on their own or with others
Where there is intentional abuse, adult safeguarding under Section 42, the Care Act, should always be considered. Work developed by ADASS, carers groups, commissioners and organisations working with carers, identify six distinct areas related to carers and safeguarding:
Partnership working: Carers have a wealth of information and knowledge about the person that they support. As well as raising concerns, carers are able to support safeguarding enquiries by sharing information and are valued partners in such enquiries. Their views may hold the key to protecting people. If a carer speaks up about abuse or neglect, it is essential that they are listened to and appropriate enquiries made Carers may identify and mitigate risk and act as advocates. The lessons from transforming care and other public inquiries need to be taken forward in viewing carers as equal partners unless there are valid reasons not to.
Prevention: Carers play a significant role in preventing the need for services and it is important that professionals consider preventing carers from developing needs for care and support themselves. There is a plethora of research findings that people who act as long-time carers, have poorer physical and mental health. Strategies that support carers to continue to care should take carer resilience into account. Listening to local carer communities about the pressures they are face should be reflected in joint strategic needs assessments. Partnership working between, health, social care and carers groups is one way of working effectively to ensure that prevention strategies reduce the incidents of safeguarding and support carers to carry out their duties safely.
Support: If a carer experiences intentional or unintentional harm from the adult they are supporting, or if a carer unintentionally or intentionally harms or neglects the adult they support, consideration should be given to whether, as part of the assessment and support planning process for the carer and, or, the adult they care for, support can be provided that removes or mitigates the risk of abuse.’ (statutory guidance 14.35). One vehicle for assessing individual need is a carer’s assessment which is distinct from a needs assessment.
Information and advice: Carers need to know how they can find support and services available in their area, and be able to access advice, information. Carers need to know, that they can raise a concern in a safe environment and be confident that their concerns will be acted upon. It might be that people are unaware that the actions that they take could be perceived by others as abusive. Carers should have access to information and advice in a way that is meaningful to them and may themselves be in need of care and support and need to know how they can access services.
Advocacy: In some instances, the most appropriate person to support the adult at risk and act as an advocate is the primary carer. Where the carer is acting in the role of advocate, they may need support to do so, therefore professionals need to provide information and ensure that it is understood. The carer themselves may be in need of an advocate.
Role of carers in strategic planning: There are two key areas that should take account of carers in safeguarding strategic plans. First, SABs should ensure their policies, procedures and practice recognise the need to support carers and also to work with carers who are experiencing or causing harm or abuse. Second, SABs should engage with carers and local stakeholders and work together for better safeguarding practice.
2.3 Types and indicators of abuse and neglect
There are 10 categories of abuse described within the Care and support statutory guidance. These categories are expansive and cover a range of abusive situations or behaviours. It is important to recognise that exploitation is a common theme in nearly all types of abuse and neglect. The Statutory Guidance (para 14.17) states that:
“Local authorities should not limit their view of what constitutes abuse or neglect, as they can take many forms and the circumstances of the individual case should always be considered; although the 3 stage criteria will need to be met before the issue is considered as a safeguarding concern”.
Type of abuse: Physical abuse
Description:Including assault, hitting, slapping, pushing, misuse of medication, restraint or inappropriate physical sanctions. In extreme circumstances unlawful or inappropriate use of restraint may constitute a criminal offence.
Restraint covers a wide range of actions. It includes the use of active or passive means to ensure that the person concerned complies.
Restrictive interventions are defined as: ‘deliberate acts on the part of other person(s) that restrict an individual’s movement, liberty and /or freedom to act independently in order to:
- take immediate control of a dangerous situation where there is a real possibility of harm to the person or others if no action is undertaken
- end or reduce significantly the danger to the person and others
- contain or limit the persons freedom for longer than is necessary’
If restrictive interventions are carried out for any other purpose than those listed above, concerns should always be escalated through safeguarding procedures (DH 2014)
Female Genital Mutilation (FGM) is a very specific form of physical (and psychological) abuse. FGM is a procedure where the female genitals are deliberately cut, injured or changed, but where there’s no medical reason for this to be done. FGM is also known as “female circumcision” or “cutting”, and by other terms such as sunna, gudniin, halalays, tahur, megrez and khitan, among others. FGM is usually carried out on young girls between infancy and the age of 15, most commonly before puberty starts. It is illegal to practice FGM in the UK and is child abuse. It is also illegal to take girls who are British Nationals or who are permanent residents of the UK abroad for FGM. There is a mandatory duty on healthcare professionals to report any identified cases of FGM in females under the age of 18 years.
FGM is very painful and can seriously harm the health of women and girls. It can also cause long-term problems with sex, childbirth and mental health.
Professionals working with women who have been subject to FGM may want to signpost them to appropriate health services for help and support. Further information, including on safeguarding women and girls at risk of FGM is available here.
Type of abuse:Domestic abuse
Description: The Home Office defines domestic abuse as: any incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse between those aged 16 or over, who are or have been intimate partners or family members regardless of gender or sexuality. This can encompass but is not limited to the following types of abuse: psychological, physical, sexual, financial, emotional abuse and ‘honour’ based violence. Further information on how to get help can be found here.
Honour Based Violence (HBV) is committed when families feel that dishonour has been brought to them. It will usually be a criminal offence and referring to the Police must always be considered. Women are predominantly (but not exclusively) the victims and the violence is often committed with a degree of collusion from family members and/or the community. Some victims of HBV may contact the Police or other organisations for help themselves. But many others are so isolated and controlled that they may be unable to seek help. Adult safeguarding concerns that may indicate HBV include domestic abuse, concerns about forced marriage, enforced ‘house-arrest’ and missing persons reports.
Forced Marriage is a term used to describe a marriage in which one or both parties are married without their freely given consent or against their will. A forced marriage differs from an arranged marriage in which both parties consent to the assistance of a third party in identifying a spouse. In a situation where there is a concern that an adult is being forced into a marriage that they cannot consent to, there will be an overlap between action taken under the forced marriage provisions and adult safeguarding processes.
If an adult safeguarding concern is raised about HBV or forced marriage, Police should be contacted as urgent action may need to be taken and they (in co-ordination with other relevant specialised organisations) have the necessary expertise to help manage the risk.
Type of abuse:Sexual abuse
Description:Including rape, indecent exposure, sexual harassment, inappropriate looking or touching, sexual teasing or innuendo, sexual photography, subjection to pornography or witnessing sexual acts, indecent exposure, sexual assault and sexual acts to which the adult has not consented or was pressured into consenting. Sexual exploitation involves situations, contexts and relationships where adults at risk receive something (e.g. food, accommodation, drugs, alcohol, cigarettes, gifts, money, affection) as a result of them performing sexual acts (and/or another/others performing such acts on them). Sexual exploitation affects men as well as women. People who are being exploited may not always perceive such behaviours as exploitation. In all cases those exploiting the adult at risk have power over them by virtue of their position, gender, age, physical strength, intellect, economic situation or other resources. There is a distinct inequality in the relationship.
Type of abuse:Psychological abuse
Description:Including emotional abuse, threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, cyber bullying, isolation, unreasonable and unjustified withdrawal of services or supportive networks.
Type of abuse:Financial or material abuse
Description: Including theft, fraud, internet scamming, coercion in relation to an adult’s financial affairs or arrangements including in connection with wills, property, inheritance or financial transactions and the misuse or misappropriation of property, possessions or benefit. An adult at risk may be persuaded to part with large sums of money/life savings.
Such concern should always be reported to the police and if relevant, local Trading Standards for further investigation. Local trading standards should be involved in the work of SABs. Where this abuse is perpetrated by someone with authority to manage the adult at risks finances, the office of the public guardian should be informed (in relation to deputies/atorneys) or the DWP (for appointees).
Such abuse may take the form of a ‘Mate Crime’. The Safety Net Project define this as occurring ‘when vulnerable people are befriended by members of the community who go on to exploit and take advantage of them. It may not be an illegal act but still has a negative effect on the individual’. Mate Crime is often difficult for the Police to investigate due to its sometimes ambiguous nature but should be reported to the Police who will decide as to if a criminal offence has been committed. Mate crime is committed by someone the adult knows and often happens in private. In recent years there have been several SARs relating to people with a learning disability who were murdered or seriously harmed by people who purported to be their friend.
Type of abuse:Modern slavery
Description:This type of abuse encompasses slavery, human trafficking, forced labour and domestic servitude.Traffickers and slave masters using whatever means they have at their disposal to coerce, deceive and force individuals into a life of abuse, servitude and inhumane treatment. Serious and organised crime gangs make significant amounts of money from human trafficking. They exploit the social, cultural and financial vulnerabilities of the person. They control almost all aspects of the person’s life with little regard for their welfare and health. However, adults who are enslaved are not always subject to trafficking. Someone is in slavery if they are forced to work through physical or mental threat, owned or controlled by an ‘employer’ (usually through abuse or threat of abuse), dehumanised and treated as a commodity (bought and sold as ‘property’), physically constrained or has restrictions placed on his/her freedom of movement. Since 2015, specific authorities have had a duty to notify the Home Office of any individual suspected as a victim of slavery or human trafficking. Further information can be found here.
Type of abuse:Discriminatory abuse
Description:This includes harassment, slurs or similar treatment because of race, gender and gender identity, age, disability, sexual orientation or religion. Examples of discriminatory abuse may include: denying access to communication aids, not allowing access to an interpreter, signer or lipreader. Harassment or deliberate exclusion on the grounds of a protected characteristic. Denying basic rights to healthcare, education, employment and criminal justice relating to a protected characteristic. Substandard service provision relating to a protected characteristic (SCIE 2015).
Some forms of discriminatory abuse may also constitute a hate crime – defined by the Crown prosecution service as “any criminal offence which is perceived by the victim or any other person, to be motivated by hostility or prejudice, based on a person’s disability or perceived disability; race or perceived race; or religion or perceived religion; or sexual orientation or perceived sexual orientation or transgender identity or perceived transgender identity.”
There is no legal definition of hostility so the police and CPS use the everyday understanding of the word which includes ill-will, spite, contempt, prejudice, unfriendliness, antagonism, resentment and dislike.
Type of abuse:Organisational abuse
Description:This includes neglect and poor care practice within an institution or specific care setting such as a hospital or care home, for example, or in relation to care provided in one’s own home. This may range from one off incidents to on-going ill-treatment. It can be through neglect or poor professional practice as a result of the structure, policies, processes and practices within an organisation.
Type of abuse: Neglect and acts of omission
Description:This includes ignoring medical, emotional or physical care needs, failure to provide access to appropriate health, care and support or educational services and/or the withholding of the necessities of life, such as medication, adequate nutrition and heating. Neglect also includes a failure to intervene in situations that are dangerous to the person concerned or to others, particularly where the adult at risk lacks the mental capacity to assess risk for themselves.
Type of abuse:Self-neglect
Description:This covers a wide range of behaviour neglecting to care for one’s personal hygiene, health or surroundings and includes behaviour such as hoarding. It should be noted that self-neglect may not always prompt a section 42 enquiry. An assessment should be made on a case by case basis. A decision on whether a response is required under safeguarding will depend on the adult’s ability to protect themselves by controlling their own behaviour. There may come a point when they are no longer able to do this, without external support.
Self neglect – Devon Safeguarding Adults Partnership.
2.4 Radicalisation
Radicalisation is the process through which people develop support for extremist political, religious or other ideas. This can lead them to support violent extremism and terrorism. People may become radicalised if their views and beliefs are influenced by extreme ideas and perspectives.
Radicalisation is a type of exploitation which often happens out of sight, leaving person experiencing the exploitation at serious risk of harm. People may be radicalised through exposure to a particular ideology, or due to non-ideological reasons – for example because of a specific grievance.
People can be radicalised by family members or friends, through direct contact with extremist groups, or through the internet, social media and online gaming sites. It can happen to anyone, although some people may be more vulnerable because of factors.
Belief in an extremist cause and membership of an extremist group can offer people a sense of purpose, identity and community. This may be particularly appealing if someone is experiencing difficulties and challenges in their life.
The UK faces a range of terrorist threats including international terrorism, Northern Ireland related terrorism and extreme right-wing terrorism. In 2018 the government set out its new Counter Terrorism Strategy (CONTEST) to reduce the risk of terrorism to the UK. Prevent is one strand of this strategy and aims to safeguard people and communities from the threat of terrorism. Prevent:
- responds to the ideological challenge we face from terrorism and aspects of extremism, and the threat we face from those who promote these views
- provides practical help to prevent people from being drawn into terrorism and ensure they are given appropriate advice and support
- works with a wide range of sectors (including education, criminal justice, faith, charities, online and health) where there are risks of radicalisation that we need to deal with
It is possible to intervene during the radicalisation process and stop someone becoming drawn towards terrorism or supporting violent extremist activity. Early detection and referral into prevent provides the best chance of stopping someone from being drawn into terrorism. Prevent referrals are screened, further information is sought, and risks are assessed. Where there are concerns about a particular individual their consent will be sought prior to entering what is known as a channel process.
It is possible to intervene during the radicalisation process and stop someone becoming drawn towards terrorism or supporting violent extremist activity. Early detection and referral into prevent provides the best chance of stopping someone from being drawn into terrorism. Prevent referrals are screened, further information is sought, and risks are assessed. Where there are concerns about a particular individual their consent will be sought prior to entering what is known as a channel process.
2.4.1 Channel Panel
Channel is a local authority led multi-agency process developed to support people at risk of being drawn towards terrorism or violent extremism.
Where appropriate, partners work collaboratively to establish a bespoke package of support for vulnerable individuals. Interventions could take the form of mentoring, welfare support, presenting opportunities to develop other interests or giving access to key services. These types of intervention can be very successful and there are examples in Torbay and Devon where they have been used to help individuals move away from a potentially destructive path.
2.5 Who abuses and neglects adults?
- spouses/partners
- other family members
- neighbours
- friends
- acquaintances
- local residents
- people who deliberately exploit adults they perceive as vulnerable to abuse
- paid staff or professionals
- volunteers and strangers
Abuse can happen anywhere: for example, in someone’s own home, in a public place, in hospital, in a care home or in college. It can take place when an adult lives alone or with others.
2.6 Serious Incident
The Serious Incident Framework should be read in conjunction with the Never Events Policy and Framework. The Serious Incident Framework is not a substitute for safeguarding. Where safeguarding is indicated a safeguarding concern must be raised, however a root cause analysis under the Serious Incident Framework may be considered an appropriate response to a safeguarding enquiry.
Examples/guidance for staff, not exhaustive, seek advice from safeguarding leads within the organisation as required:
- an NHS organisation identifies a safeguarding concern, for example through staff at Accident and Emergency seeing signs of physical abuse. This may warrant a safeguarding concern being raised to the Local Authority but would not be routinely recorded as an Serious Incident (SI)
- if there are allegations against healthcare staff of a healthcare provider of an adult at risk, then a safeguarding concern would need to be raised. An SI would need to be declared if the criteria for an SI were also met. Equally where there is patient against patient abuse an SI would need to be declared if the criteria for a SI was also met
- lastly, there are SIs that are not safeguarding adult concerns for example a pressure ulcer that was unavoidable. SI investigations will still be undertaken but without raising a safeguarding adult concern. This is obviously dependent on the situation and throughout the incident investigation there needs to be consideration of acts of omission and/or neglectful care – as a safeguarding adult concern would need to be raised in these incidences.
2.7 Safeguarding Adult Review(s) (SARs)
Section 44, the Care Act 2014 stipulates that SABs must arrange a SAR when there is concern that the SABs or partner agencies could have worked more effectively to safeguard an adult in its area with care and support needs, in two situations:
1. The adult dies as a result of abuse or neglect, whether known or suspected.
2. The adult has not died, but the SABs knows or suspects that the adult has experienced serious abuse or neglect.
Section 3: Adult safeguarding practice
This section sets out the essential work that must be considered throughout adult safeguarding. In every case there must be evidence of due diligence and attention to mental capacity and consent.
3.1 Mental Capacity Act (2005)
The Mental Capacity Act 2005 provides a statutory framework to empower and protect people who may lack capacity to make decisions for themselves; and establishes a framework for making decisions on their behalf. This applies whether the decisions are life-changing events or everyday matters. All decisions taken in the adult safeguarding process must comply with the Act.
The Mental Capacity Act outlines five statutory principles that underpin the work with adults who may lack mental capacity:
- a person must be assumed to have capacity unless it is established that he lacks capacity
- a person is not to be treated as unable to make a decision unless all practicable steps to help him to do so have been taken without success
- a person is not to be treated as unable to make a decision merely because he makes an unwise decision
- an act done, or decision made, under this Act for or on behalf of a person who lacks capacity must be done, or made, in his best interests
- before the act is done, or the decision is made, regard must be had to whether the purpose for which it is needed can be as effectively achieved in a way that is less restrictive of the person’s rights and freedom of action.
Learning from SARs continues to show that staff working with adults who lack mental capacity are not fully complying with principle 5 above.
The majority of adults that require additional safeguards are people who are likely to lack mental capacity to make decisions about their care and support needs.
Mental Capacity refers to the ability to make a decision about a particular matter at the time the decision is needed. It is always important to establish the mental capacity of an adult who is at risk of abuse or neglect, should there be concerns over their ability to give informed consent to:
- planned interventions and decisions about their safety
- their safeguarding plan and how risks are to be managed to prevent future harm
3.1.1 Mental Capacity Assessment
The Act says that:
‘…a person lacks capacity in relation to a matter if at the material time he/she is unable to make a decision for him/herself in relation to the matter because of an impairment of, or disturbance in the functioning of the mind or brain. Further, a person is not able to make a decision if they are unable to:
- understand the information relevant to the decision
- retain that information long enough for them to make the decision
- use or weigh that information as part of the process of making the decision
- communicate their decision (whether by talking, using sign language or by any other means such as muscle movements, blinking an eye or squeezing a hand)
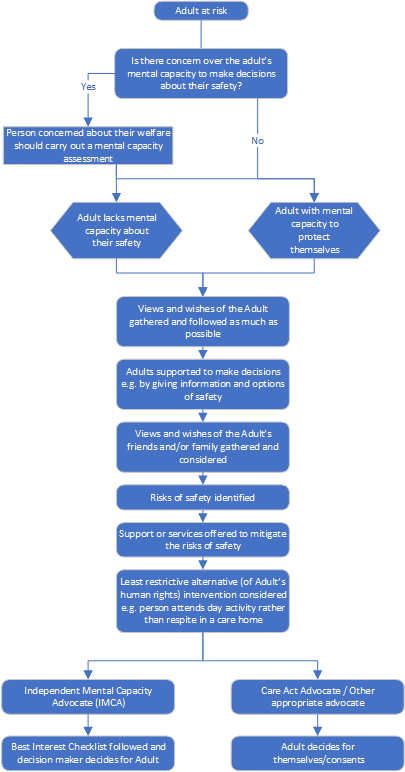
Mental capacity is time and decision specific. This means that an adult may be able to make some decisions at one point but not at other points in time. Their ability to make a decision may also fluctuate over time. If an adult is subject to coercion or undue influence by another person this may impair their judgement and could impact on their ability to make decisions about their safety. Thus, an adult could be put under pressure, for example in domestic abuse situations, that they lack the mental capacity to make the decisions about their safety. Staff must satisfy themselves that the adult has the mental ability to make the decision themselves, if not, it is best to err on the side of caution, identify the risks and consider support or services that will mitigate the risk. Preventing the person from isolation can be a protective factor. Involving an advocate could assist in such circumstances. Advocacy support can be invaluable and may be provided by an Independent Mental Capacity Advocate (IMCA) or another appropriate advocate.
3.1.2 Consent in relation to safeguarding
The Care and Support Statutory Guidance chapter 14 advises that the first priority in safeguarding should always be to ensure the safety and well-being of the adult.
Making Safeguarding Personal is a person-centred approach which means that adults are encouraged to make their own decisions and are provided with support and information to empower them to do so. This approach recognises that adults have a general right to independence, choice and self-determination including control over information about themselves. Staff should strive to deliver effective safeguarding consistently with both of the above principles. They should ensure that the adult has accessible information so that the adult can make informed choices about safeguarding: what it means, risks and benefits and possible consequences. Staff will need to clearly define the various options to help support them to make a decision about their safety.
Adults may not give their consent to the sharing of safeguarding information for a number of reasons. For example, they may be unduly influenced, coerced or intimidated by another person, they may be frightened of reprisals, they may fear losing control, they may not trust social services or other partners, or they may fear that their relationship with the abuser will be damaged. Reassurance and appropriate support may help to change their view on whether it is best to share information. Staff should consider the following and:
- explore the reasons for the adult’s objections – what are they worried about?
- explain the concern and why you think it is important to share the information
- tell the adult with whom you may be sharing the information with and why
- explain the benefits, to them or others, of sharing information – could they access better help and support?
- discuss the consequences of not sharing the information – could someone come to harm?
- reassure them that the information will not be shared with anyone who does not need to know
- reassure them that they are not alone, and that support is available to them.
If, after this, the adult refuses intervention to support them with a safeguarding concern, or requests that information about them is not shared with other safeguarding partners, in general, their wishes should be respected. However, there are a number of circumstances where staff can reasonably override such a decision, including:
- the adult lacks the mental capacity to make that decision – this must be properly explored and recorded in line with the Mental Capacity Act
- emergency or life-threatening situations may warrant the sharing of relevant information with the emergency services without consent
- other people are, or may be, at risk, including children
- sharing the information could prevent a serious crime
- a serious crime has been committed
- the risk is unreasonably high
- staff are implicated
- there is a court order or other legal authority for taking action without consent
In such circumstances, it is important to keep a careful record of the decision-making process. Staff should seek advice from managers in line with their organisations’ guidance before overriding the adult’s decision, except in emergency situations. Managers should make decisions based on whether there is an overriding reason which makes it necessary to take action without consent and whether doing so is proportionate because there is no less intrusive way of ensuring safety. Legal advice should be sought where appropriate. If the decision is to take action without the adult’s consent, then unless it is unsafe to do so, the adult should be informed that this is being done and of the reasons why.
If none of the above apply and the decision is not to share safeguarding information with other safeguarding partners, or not to intervene to safeguard the adult:
- support the adult to weigh up the risks and benefits of different options
- ensure they are aware of the level of risk and possible outcomes
- offer to arrange for them to have an advocate or peer supporter
- offer support for them to build confidence and self-esteem if necessary
- agree on and record the level of risk the adult is taking
- record the reasons for not intervening or sharing information
- regularly review the situation
- try to build trust to enable the adult to better protect themselves
It is important that the risk of sharing information is also considered. In some cases, such as domestic violence or hate crime, it is possible that sharing information could increase the risk to the adult. Safeguarding partners need to work jointly to provide advice, support and protection to the adult in order to minimise the possibility of worsening the relationship or triggering retribution from the abuser.
3.2 Advocacy and support
3.2.1 Advocacy
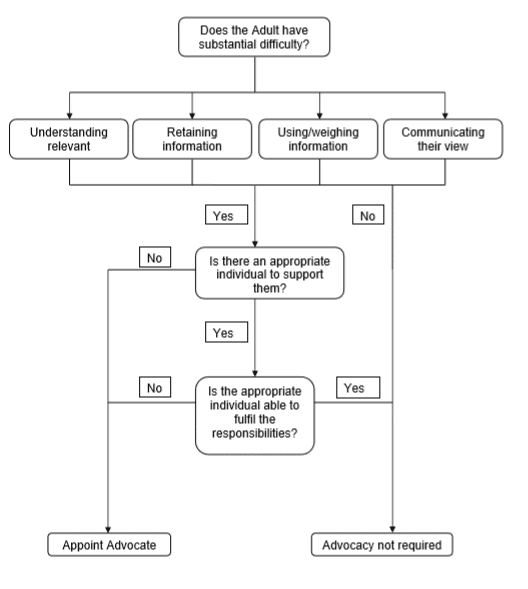
The Care Act 2014 requires that a Local Authority must arrange, where appropriate, for an independent advocate to represent and support an adult who is the subject of a safeguarding enquiry or SAR where the adult has ‘substantial difficulty’ in being involved in the process and where there is no other appropriate individual to help them (Section 68).
There are distinct differences between an Independent Mental Capacity Advocate (IMCA) introduced under the Mental Capacity Act 2005, and an Independent Advocate introduced under the Care Act 2014. Independent advocates cannot undertake advocacy services under the Mental Capacity Act 2005, however where there is an appointed IMCA they may also take on the role of Independent Advocate under the Care Act 2014.
The following flowchart illustrates the interface between mental capacity and advocacy. It should be remembered that where the adult does not want support from family or friends that their wishes should be respected, and an independent advocate provided. Further information on advocacy requirements under the Care Act is accessible here.
3.2.2 Support to adults
A requirement under the Equality Act 2010 is for provision and adjustments to enable disabled people equal access to information and advice. Ensuring equality may reduce or remove substantial difficulty. Access to other services for example, translators should always be considered to ensure that the adults are afforded every opportunity to participate and be involved.
3.3 Managing risk
TDSAP organisations will have a range of internal risk assessment tools available. These tools support staff to evidence professional judgement during their decision making. Issues around information sharing may be relevant in this context.
3.3.1 Involving the adult
Making Safeguarding Personal stresses the importance of keeping the adult at the centre of positive approaches to managing risks to their safety. Under MSP the adult is best placed to identify risks, provide details of its impact and whether or not they find the mitigation acceptable. Working with the adult to lead and manage the level of risk that they identify as acceptable creates a culture where:
- adults feel more in control
- adults are empowered and have ownership of the risk
- there is improved effectiveness and resilience in dealing with a situation
- there are better relationships with professionals
- good information sharing to manage risk, involving all the key stakeholders
- key elements of the person’s quality of life and well-being can be safeguarded
3.3.2 Identifying risk
Not every situation or activity will entail a risk that needs to be assessed or managed. The risk may be minimal and no greater for the adult, than it would be for any other person. Risks:
- can be real or potential
- can be positive or negative
- should take into account all aspects of an individual’s wellbeing and personal circumstances
Sources of risk might fall into one of the four categories below:
- private and family life: The source of risk might be someone like an intimate partner or a family member
- community based risks: This includes issues like ‘mate crime’, anti-social behaviour, and gang-related issues
- risks associated with service provision: This might be concerns about poor care which could be neglect or organisational abuse, or where a person in a position of trust because of the job they do financially or sexually exploits someone
- self-neglect: Where the source of risk is the person themselves.
3.3.3 Risk assessment
Risk assessment involves collecting and sharing information through observation, communication and investigation. It is an on-going process that involves persistence and skill to assemble and manage relevant information in ways that are meaningful to all concerned. Risk assessment that includes the assessment of risks of abuse, neglect and exploitation of people should be integral in all assessment and planning processes, including assessments for self-directed support and the setting up of personal budget arrangements. Assessment of risk is dynamic and on-going and a flexible approach to changing circumstances is needed. The primary aim of a safeguarding adult’s risk assessment is to assess current risks that people face and potential risks that they and other adults may face. Specific to safeguarding, risk assessments should encompass:
- the views and wishes of the adult
- the person’s ability to protect themselves
- factors that contribute to the risk, for example, personal, environmental
- the risk of future harm from the same source
- identification of the person causing the harm and establishing if the person causing the harm is also someone who needs care and support
- deciding if domestic abuse is indicated and the need for a referral to a MARAC
- deciding if a community multi-agency risk assessment (high risk panel) is needed
- identify people causing harm
- if it may increase risk where information is not shared
Mechanisms to support adult safeguarding are detailed in TDSAP Multi-Agency Frameworks for Managing Risk guidance. This provides key information needed for professionals on the structure and contact points for the main multi-agency frameworks for managing risk posed by and to adult’s resident in Torbay and Devon.
3.3.4 Risk management
The focus must be on the management of risks not just a description of risks. Employers need to take responsibility for the management of risk within their own organisation and share information responsibly where others may be at risk from the same source. The local authority may be ultimately accountable for the quality of section 42(2) enquiries, but all organisations are responsible for supporting holistic risk management, with the adult and in partnership with other agencies.
It is the collective responsibility of all organisations to share relevant information, make decisions and plan intervention with the adult. A plan to manage the identified risk and put in place safeguarding measures includes:
- what immediate action must be taken to safeguard the adult and/others
- who else needs to contribute and support decisions and actions; What the adult sees as proportionate and acceptable
- what options there are to address risks
- when action needs to be taken and by whom
- what the strengths, resilience and resources of the adult are
- what needs to be put in place to meet the on-going support needs of the adult
- what the contingency arrangements are
- how will the plan be monitored.
Positive risk management needs to be underpinned by widely shared and updated contingency planning for any anticipated adverse eventualities. This includes warning signs that indicate risks are increasing and the point at which they become unacceptable and therefore trigger a review.
Effective risk management requires exploration with the adult using a person-centred approach, asking the right questions to build up a full picture. Not all risks will be immediately apparent; therefore, risk assessments need to be regularly updated as part of the safeguarding process and possibly beyond.
3.3.5 Reviewing risk
Individual need will determine how frequently risk assessments are reviewed and wherever possible there should be multi-agency input. These should always be in consultation with the adult at risk.
3.3.6 Risk disputes
Throughout these policies and procedures risk assessment and risk management is carried out in partnership with the adult, wider support network and others. The decision to involve others or not is in itself a decision which may give rise to risk, and the individual may need support to make this decision.
The professional views of risk may differ from the views of the adult. Perceived risks have implications for the safety and the independence of the individual, but they also have implications for the accountability of professionals. This highlights the importance of training and/or regular practice in making independent decisions by adults. Accessible knowledge through information and advice, assertiveness through the right kind of advocacy and support may be appropriate.
Professionals need to embrace and support positive risk taking by finding out why the person wishes to make a particular choice, what this will bring to their life, and how their life may be adversely affected if they are not supported in their choice.
The promotion of choice and control, of more creative and positive risk-taking, implies greater responsibility on the part of the adult and greater emphasis on keeping them at the centre of decision making.
It may not be possible to reach agreement, but professionals need to evidence that all attempts to reach agreement were taken. Where there are concerns about people making unwise decisions, or there is high risk that requires wider collaboration; a Multi-Agency High Risk Forum such as Creative Solutions is one model used to support safeguarding adults’ processes.
Other models include risk enablement meetings, where there is an emphasis on shared responsibility, including the adult at risk, and advocate. A risk enablement meeting should only be convened as a last resort.
3.4 Recording actions under adult safeguarding
A record of all actions and decisions must be made, as record keeping is a vital component of professional practice and is an essential element in documenting the legal justification for decisions. When abuse or neglect is raised, managers need to look for past incidents, concerns, risks and patterns. We know that in many situations, abuse and neglect arise from a range of incidents over a period of time. In the case of providers registered with CQC, records of these should be available to service commissioners and the CQC so they can take the necessary action. At a minimum there should be an audit trail of:
- date and circumstances of concerns and subsequent action
- decision making processes and rationales
- risk assessments and risk management plans
- consultations and correspondence with key people
- advocacy and support arrangements
- safeguarding plans
- outcomes
- feedback from the adult and their personal support network
- differences of professional opinion
- referrals to professional bodies.
As records may be disclosed in courts in criminal or civil actions and to individuals under data protection legislation, all organisations should audit safeguarding concerns and outcomes as part of their quality assurance (local authority should use existing codes within the safeguarding adult collections categories). Supervisors should ensure that recording is addressed in supervision and that staff are clear of their responsibilities. SABs should regularly review the quality of recording as part of their performance and quality data scrutiny.
Learning lessons from past mistakes and missed opportunities highlighted in SARs and other reports emphasise the need for quality recording especially when managing abuse, neglect and risk. This includes providing rationales for actions and decisions, whether or not they were taken, and if not the reasons for this.
Quality recording of adult safeguarding not only safeguards adults, but also protects workers by evidencing decision making based on the information available at the time. For more information see the University of the West of England advice on the importance of keeping records.
3.5 Organisational learning
It is essential that all aspects of safeguarding practice are monitored and scrutinised on a regular basis. All staff have a responsibility to audit their work and a set of local outcome focused standards might support staff.
All agencies need to take responsibility for organisational learning and implement changes to their practice as a result of audits, complaints, SARs, and most importantly feedback from adults at risk about what works well and what needs to improve provide opportunities for learning from themes and patterns of practice that can add value to learning from good practice and pinpointing necessary changes.
In addition to practice guidance highlighted throughout this document, staff may find the following information from SCIE helpful on adult safeguarding questions.
Section 4: Adult safeguarding procedures
4.1 Context
The main objective of adult safeguarding procedures is to provide guidance to mitigate against the risks to adults from abuse or neglect, ensuring that any outcomes from an enquiry are client focused and achievable and identify immediate action to be taken where required.
The procedures are a means for staff to combine principles of protection and prevention with individuals’ self-determination, respecting their views, wishes and preferences in accordance with MSP. They are a framework for managing safeguarding interventions that are fair and just, through strong multi-agency partnerships that provide timely and effective prevention of and responses to abuse and neglect. All organisations who work with or support adults experiencing, or who are at risk of, abuse and neglect may be called upon to lead or contribute to a safeguarding enquiry and need to be prepared to take on this responsibility.
Guidance is often criticised for over‐standardising practice and undervaluing the skills required when applying policies in diverse circumstances. The key focus is on using professional skills to ensure safeguarding is personalised and the outcomes and goals from any enquiry are client focused, realistic and attainable.
4.2 The four stage process
The procedures chapter has been structured within a four stage process:
- concerns
- enquiry
- safeguarding plan and review
- closing the enquiry
4.3 Roles and responsibilities
Before going through each stage of the process in depth, Appendix 1: Safeguarding Adults Structures and organisations will define roles and responsibilities and provides context within which the procedures operate.
4.3.1 Safeguarding adult concern referral points
Each organisation must have its own operational guidance on how it manages adult safeguarding concerns, including a list of referral points with up-to-date contact details, so that staff and the public know how to report abuse and neglect. The local authority is the main referral point even if others have their own.
4.3.2 Dealing with repeat allegations
All concerns should be considered on their own merit and recorded individually. An adult who makes repeated allegations that have been investigated and decided to be unfounded should be treated without prejudice. Where there are patterns of similar concerns being raised by the same adult within a short time period, a risk assessment and risk management plan should be developed, and a local process agreed between the agency involved with the adult making repeat allegations and the Local Authority, for responding to further concerns of the same nature from the same adult. All organisations are responsible for recording and noting where there are such situations and may be asked to contribute to a multi-agency response. Information sharing to assess and analyse data is essential to ensure that adults are safeguarded, and an appropriate response is made. Staff should also be mindful of public interest issues.
In considering how to respond to repeated concerns the following factors need to be considered:
- the safety of the adult who the concern is about
- mental capacity and ability of the individual’s support networks to raise the concern, or to increase support to meet outcomes of safeguarding concerns
- wishes of the adult at risk and impact of the concern on them
- impact on important relationships
- level of risk
4.3.3 People in a position of trust
While the Care Act outlines clear legal duties on the local authority to undertake enquiries in certain circumstances where adults with care and support needs are identified as experiencing or being at risk of abuse or neglect, the Care Act does not set out any primary legal duties on the local authority associated with managing allegations against people who work in a position of trust with adults with care and support needs. However, if an adult at risk has allegedly been harmed or neglected by a person in a position of trust an adult safeguarding enquiry must be carried out. Other processes, including police criminal investigation or employer’s disciplinary processes, will also be considered. All risk assessments and subsequent actions must be carefully coordinated and take account of the well-being and safety of the adult at risk. If no adult at risk has been harmed adult safeguarding processes are not required. Please refer to TDSAP Allegations Against People in Position of Trust (PiPoT) Protocol.
4.3.4 Dispute resolution and escalation
Professional disagreements should be resolved at the earliest opportunity, ensuring that the safety and wellbeing of the adult at risk remains paramount. Challenges to decisions should be respectful and resolved through co-operation. Disagreements can arise in a number of areas and staff should always be prepared to review decisions and plans with an open mind. Assurance that the adult at risk is safe takes priority. Disagreements should be talked through and appropriate channels of communication established to avoid misinterpretation.
In the event that operational staff are unable to resolve matters, more senior managers should be consulted. Please refer to TDSAP Safeguarding Adults Escalation Protocol.
4.3.5 Cross-boundary and inter-authority adult safeguarding enquiries
Risks may be increased by complicated cross-boundary arrangements, and it may be dangerous and unproductive for organisations to delay action due to disagreements over responsibilities. The rule for managing safeguarding enquiries is that the local authority for the area where the abuse occurred has the responsibility to carry out the duties under Section 42 Care Act 2014, but there should be close liaison with the placing authority.
The ‘placing authority’ continues to hold responsibility for commissioning and funding a placement. However, many people at risk live in residential settings outside the area of the placing authority. In addition, a safeguarding incident might occur during a short-term health or social care stay, or on a trip, requiring police action in that area or immediate steps to protect the person while they are in that area.
The initial lead in response to a safeguarding concern should always be taken by the local authority for the area where the incident occurred. This might include taking immediate action to ensure the safety of the person or arranging an early discussion with the police when a criminal offence is suspected.
4.4 Timescales
The adult safeguarding procedures do not set definitive timescales for each element of the process; however, target timescales are indicated. In addition, individual local authorities or SABs may make decisions on timescales for their own performance monitoring. Local guidance on timescales should reflect the ethos of the MSP agenda. It is important that timely action is taken, whilst respecting the principle that the views of the adult at risk are paramount. It is the responsibility of all agencies to proactively monitor concerns/enquiries to ensure that drift does not prevent timely action and place people at further risk. Divergence from any target timescales may be justified where:
- adherence to the agreed timescales would jeopardise achieving the outcome that the adult at risk wants
- it would not be in the best interests of the adult at risk
- significant changes in risk are identified that need to be addressed
- supported decision making may require an appropriate resource not immediately available
- persons’ physical, mental and/or emotional wellbeing may be temporarily compromised
The timescales are indicative to avoid drift but need to take account the needs and wishes of the adult/s at risk and/or other investigations such as NHS Serious Incidents (SI).
Indicative timescales
Stage one:concerns
Referring a concern
The referrer to ensure action is taken to protect the adult from harm as soon as possible and inform the Local Authority. In cases of emergency this may require the need to contact emergency services such as the Police.
The referrer to ensure they start conversations with the adult at risk, in line with MSP principles establishing their wishes and preferred outcome from raising a safeguarding concern. If the person lacks capacity, to consider whether the concern needs to be raised in their best interest.
Triaging the concern
Concerns triaged by the Local Authority, outcomes decided, and feedback provided within 2 working days.
Stage two:enquiries
Establishing preferred outcomes
Same day enquiry received if not already taken place.
First safeguarding enquiry discussion/meeting
Within 7 working days.
Second safeguarding enquiry meeting
Target time within 30 working days from start of the enquiry.
Stage three: Safeguarding plan and review
Safeguarding plan
Withing 5 working days of enquiry findings.
Review
Not more than 3 months, but dependent upon risk.
Stage four: Closing the enquiry
Actioned immediately following decision to close where possible. Other actions within 5 working days.
Stage 1: Concerns
5.1 What is an adult safeguarding concern?
An adult safeguarding concern is any worry about an adult who has or appears to have care and support needs, that they may be subject to, or may be at risk of, abuse and neglect and may be unable to protect themselves against this. The adult does not need to be already in receipt of care and support. A concern may be raised by anyone, and can be:
- an active disclosure of abuse by the adult, where the adult tells a member of staff that they are experiencing abuse and/or neglect
- a passive disclosure of abuse where someone has noticed signs of abuse or neglect, for example clinical staff who notice unexplained injuries
- an allegation of abuse by a third party, for example a family/friend or neighbour who have observed abuse or neglect or have been told of it by the adult
- a complaint or concern raised by an adult or a third party who doesn’t perceive that it is abuse or neglect. Complaint officers should consider whether there are safeguarding matters
- a concern raised by staff or volunteers, others using the service, a carer or a member of the public
- an observation of the behaviour of the adult at risk
- an observation of the behaviour of another
Concerns can be raised using the Torbay and Devon Safeguarding Adult Concern Referral Form, by telephone, email, or letter.
5.2 Police engagement
Staff contact with the police will fall mainly into four main areas:
- Reporting a crime: If an individual witnesses a crime, they have a duty to report it to the police via 999 if an emergency or for non-emergency via 101 or online reporting service
- Third party reporting of a crime: If an individual is made aware of a crime, they should support the adult at risk to report to the police or make a best interest decision to do so if the adult at risk lacks mental capacity. In domestic abuse situations practitioners should be aware of the principles of ‘Safe Enquires’ (see domestic abuse and safeguarding adults)
- Consultation with the police: Seeking advice
- Sharing intelligence and managing risk in line with agreed information sharing protocols. For example, sharing the information could prevent a crime or the risk is unreasonably high.
Where the safeguarding concerns arise from abuse or neglect deliberately intended to cause harm, then it will not only be necessary to immediately consider what steps are needed to protect the adult but also how best to report as a possible crime. Early consultation with the police is vital to support the criminal investigation.
Immediate action by the person raising the concern
The responsibility first and foremost is to safeguard the adult at risk.
a. Make an evaluation of the risk and take steps to ensure that the adult is in no immediate danger
b. Arrange any medical treatment. (note that offences of a sexual nature will require expert advice from the police)
c. If a crime is in progress or life is at risk, dial emergency services – 999
d. Encourage and support the adult to report the matter to the police if a crime is suspected and not an emergency situation
e. Take steps to preserve any physical evidence if a crime may have been committed, and preserve evidence through recording
f. Ensure that other people are not in danger
g. If you are a paid employee, inform your manager. Report the matter internally through your internal agency reporting procedures (e.g. NHS colleagues may still need to report under clinical governance or serious incident processes, report to HR department if an employee is the source of risk)
Record the information received, risk evaluation and all actions.
Manager of the person raising the concern
a. Clarify that the adult is safe, that their views have been clearly sought and recorded and that they are aware of what action will be taken
b. Check that issues of consent and mental capacity have been addressed
c. If a person’s wishes are being overridden, check that this is appropriate and that the adult understands why
d. Contact MASH if a child or young person is also at risk
e. If the person allegedly causing the harm is also an adult at risk, arrange appropriate care and support
f. Make sure action is taken to safeguard other people
g. Take any action in line with allegation/disciplinary procedures; including whether it is appropriate to suspend staff or move them to alternative duties
h. If your service is registered with the Care Quality Commission, and the incident constitutes a notifiable event, complete and send a notification to CQC
i. In addition, if a criminal offence has occurred or may occur, contact the Police
j. Preserve forensic evidence
k. Concerns about radicalisation, violent extremism or terrorism make a referral to prevent@devonandcornwall.pnn.police.uk
l. Consider if the case should be put forward for a SAR
m. Record the information received and all decisions and actions taken.
5.3 Referring a concern to the local authority
The Care Act 2014 Section 42(1) states a safeguarding concern must be raised to the local authority if, on the basis of the information available, there is reasonable cause to suspect that an adult:
- has needs for care and support (whether or not the local authority is meeting any of those needs)
- is experiencing, or at risk of abuse or neglect
- as a result of their care and support needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect
Decisions need to take into account all relevant information that is available, including the views of the adult in all circumstances where it is possible and safe to seek their views. The person referring an adult safeguarding concern must ensure that they have sought consent from the adult at risk to make the referral, or if lacking capacity that in doing so would be in their best interest. Identifying the adult at risk preferred outcomes is best practice when making the referral and must be explored with them where possible.
If the adult does not want to pursue matters through safeguarding action, staff should be sure that the adult is fully aware of the consequences of their decisions, and that all options have been explored and that not proceeding further is consistent with legal duties.
There may be some occasions when the adult at risk does not want to pursue a concern being raised to the Local Authority. If possible, the adult at risk’s wishes should be respected and other ways of ensuring the adult’s safety explored. Where there is a potentially high-risk situation, staff should be vigilant of possible coercion and the emotional or psychological impact that the abuse may have had on the adult.
Decision makers also need to take account of whether or not there is a public or vital interest to refer the concern to the Local Authority. Where there is a risk to other adults, children or young people or there is a public interest to take action because a criminal offence had occurred, and the view is that it is a safeguarding matter, the wishes of the individual may be overridden. Where the sharing of information to prevent harm is necessary, lack of consent to information sharing can also be overridden. This should include where the adult at risk is deceased or the alleged perpetrator is a professional.
In the event that people lack the capacity to provide consent, action should be taken in line with the Mental Capacity Act 2005. Please refer to Practice in Section 3.
Good practice guidance – disclosure
- speak in a private and safe place
- accept what the person is saying
- don’t ‘interview’ the person; but establish the basic facts avoiding asking the same questions more than once
- ask them what they would like to happen and what they would like you to do
- don’t promise the person that you’ll keep what they tell you confidential; explain who you will tell and why
- if there are grounds to override a person’s consent to share information, explain what these are
- explain how the adult will be involved and kept informed
- provide information and advice on keeping safe and the safeguarding process
- make a best interest decision about the risks and protection needed if the person lacks capacity to consent.
Establish:
- the risks and what immediate steps to take
- whether an interpreter or other support is needed to aid communication
- whether it is likely that advocacy may be required
- personal care and support arrangements
- mental capacity to make decisions about whether the adult is able to protect themselves and consent to the safeguarding process
Concerns checklist
- safety of adult and others made
- initial conversation held with the adult
- emergency services contacted and recorded
- medical treatment sought
- consent sought
- mental capacity considered
- best interest decisions made and recorded
- public and vital interest considered and recorded
- police report made
- evidence preserved
- referrals to specialist agencies e.g. channel
- referral to children services if there are child and young people safeguarding matters
- action taken to remove/reduce risk where possible and recorded
- recorded clear rationales for decision making
- referral to local authority included relevant information.
There is one point of contact team who triage concerns within Torbay:
Torbay Safeguarding Adults Single Point of Contact Team (SPOC)
Address: 4th Floor, Union House, Union Street, Torquay, TQ1 3YA
Telephone: 01803 219888 (Professionals only) 01803 219700 (Public line)
Email: safeguarding.alertstct@nhs.net
There is one single service who triage Concerns within Devon County Council:
Devon Safeguarding Adults Services
1st Floor, The Annexe, County Hall, Exeter, EX2 4QD
Telephone: 0345 1551 007
Email: adultsc.safeguardingadultservices-mailbox@devon.gov.uk
In Devon, Safeguarding concerns raised by members of the public should be referred by calling Adult Social Care on: 0345 1551 007 or you can email:
Email: adultsc.safeguardingadultservices-mailbox@devon.gov.uk
The operational times of the Safeguarding Adults Hubs (excluding bank holidays) are: Monday – Thursday 9.00 am to 5.00 pm, Friday 9.00 am to 4.30 pm
Outside of these times callers will be referred to Devon County Council’s Emergency Duty Service (EDS) 0345 6000 388 or Torbay Emergency Duty Service 0300 456 4876.
5.4 Feedback on safeguarding concerns raised
All adult safeguarding concerns referred to the Local Authority should be assessed to decide if the duty to carry out a safeguarding adult enquiry is met. Keeping the person who raised the concern informed is an essential requirement under these policies and procedures. Feedback must be provided to all those raising concerns as this provides assurance that action has been taken whether under adult safeguarding or not. It is, however, important that feedback to the wider community needs to take account of confidentiality and requirements of data protection legislation. It is more likely that the public will continue to raise concerns, where there is an acknowledgement that their concern has reached the right agency and is being taken seriously.
Organisations raising concerns may want to challenge or discuss decisions and need to be updated on what action has been taken.
Stage 2:Enquiry
6.1 What is an adult safeguarding enquiry?
Under the Care Act 2014 Section 42(1) informs the decision identifying a duty to make enquiries under section 42(2). When the local authority receives a safeguarding adult concern it is responsible for this public law decision as to whether or not to proceed with the duty to make enquiries under section 42(2). That is to ‘make (or cause to be made) whatever enquiries it thinks necessary to enable it to decide whether any action should be taken in the adult’s case (whether under this part or otherwise) and, if so, what and by whom.’
Where the circumstances are not such as to trigger the section 42(2) safeguarding duty, the local authority may choose to carry out proportionate safeguarding enquiries, in order to promote the adult’s well-being and to support preventative action. An enquiry should establish whether and what action needs to be taken to prevent or stop abuse or neglect.
6.2 Role of the local authority
The local authority should decide very early on in the process who is the best person/organisation to lead on the enquiry. The local authority retains the responsibility for ensuring that the enquiry is referred to the right place and is acted upon.
The enquiry will be allocated to a professional, who has completed training at the appropriate level for the role they are undertaking in completing the safeguarding enquiry activities, with support and oversight from a manager who has responsibility for ensuring appropriate professional supervision is being provided.
If the local authority has asked someone else to make enquiries, it is able to challenge the organisation/individual making the enquiry if it considers that the process and/or outcome is unsatisfactory. In some circumstances the local authority may request exception reports from the manager with oversight of the safeguarding activities where an enquiry has remained open for 90 days or more. This should provide the rationale for the enquiry remaining open at that point and also assurance that measures have been taken to safeguard the individual/s in the meantime. In exceptional cases, the local authority may undertake an additional enquiry, for example, if the original fails to address significant issues.
The degree of involvement of the local authority will vary from case-to-case, but at a minimum must involve quality assurance of the enquiry undertaken.
6.3 Criminal investigation
Although the local authority has the lead role in making enquiries or requesting others to do so, where criminal activity is suspected, early involvement of the police is essential. Police investigations should be coordinated with the professional completing the safeguarding activity and the manager with oversight who may support other actions but should always be police led.
6.3.1 Ill treatment and wilful neglect
The police will determine whether there should be criminal investigations of people in positions of trust where there is ill treatment and wilful neglect. There are a number of possible offences which may apply, including the specific offences mentioned below.
Section 44 Mental Capacity Act 2005 makes it a specific criminal offence to wilfully ill-treat or neglect a person who lacks capacity.
Section 127 Mental Health Act 1983 creates an offence in relation to staff employed in hospitals or mental health nursing homes where there is ill-treatment or wilful neglect.
Sections 20 to 25 of the Criminal Justice and Courts Act 2015 relate to offences by care workers and care providers including wilful ill treatment and neglect.
6.4 Conversations with the adult (including appropriate support)
In the majority of cases, unless it is unsafe to do so each enquiry will start with a conversation with the adult at risk. Points to consider:
- the pace of conversations
- whether the presenting issue identifies the risk to the adult’s safety, or whether there are additional risks to be considered
- wider understanding and assessment of the adult overall wellbeing
The adult should be aware at the end of the conversation what action will be taken and provided with contact details for key people.
6.5 Objectives
- establish the facts
- ascertain the adult’s views and wishes and preferred outcomes
- assess the needs of the adult for protection, support and redress and how these might be met
- protect the person from the abuse and neglect, in accordance with the wishes of the adult where possible
- enable the adult to achieve resolution where possible
- wider potential risk to other adults to be considered.
Staff need to handle enquiries in a sensitive and skilled way to ensure minimal distress to the adult and where information is already known people should not have to tell their story again, this doesn’t prevent clarification being sought where necessary. There is a skill involved in eliciting information and asking the right questions, to ascertain what the concern is, how it impacts on the adult at risk, what action they would find acceptable and the level of associated risk. Whilst it is essential to put the adult at risk at ease, and to build up a rapport, the objectives of an enquiry should focus the conversation (See Good Practice Guidance)
6.6 Desired outcomes identified by the adult
The desired outcome by the adult at risk should be clarified and confirmed at the end of the conversation(s), to:
- ensure that the outcome is achievable
- manage any expectations that the adult at risk may have
- give focus to the enquiry.
Staff should support adults at risk to think in terms of realistic outcomes but should not restrict or unduly influence the outcome that the adult would like. Outcomes should make a difference to risk, and at the same time satisfy the persons’ desire for justice and enhance their wellbeing.
The adult’s views, wishes, and desired outcomes may change throughout the course of the enquiry process. There should be an on-going dialogue and conversation with the adult to ensure their views and wishes are gained as the process continues, and enquiries re-planned should the adult change their views.
Initial action and decision making under section 42 (2)
Action (if not already done)
- establish the adult is safe
- establish need for advocacy
- establish consent and capacity to make relevant decisions by understanding the management of risk, what a safeguarding enquiry is, how they might protect themselves
- establish whether the adult is aware of the safeguarding concerns and if they perceive it as a concern and want action/support
- is there suspicion that a crime may have been committed and a report to the police needed
- the adult at risk desired outcome is established
- record all actions and conversations
Decision
- who is best placed to speak with the adult at risk
- are there any reasons to delay speaking with the adult at risk
- what the safeguarding enquiry might consist of
- whether to proceed without consent
- what follow-up action may be needed
- whether actions so far have completed the enquiry
Talking through an enquiry may result in resolving it, if not, the duties under section 42(2) continue. If the adult has capacity and expresses a clear and informed wish not to pursue the matter further, the local authority should consider whether it is appropriate to end the enquiry. It should consider whether it still has reasonable cause to suspect that the adult is at risk and whether further enquiries are necessary before deciding whether further action should be taken. The adult’s consent is not required to take further steps, but the local authority must bear in mind the importance of respecting the adult’s own views. This decision must be made by the local authority by checking with the adult and consulting with relevant partners and advocate.
6.7 Planning an enquiry under section 42 (2) duties
All enquiries need to be planned and co-ordinated and key people identified. No agency should undertake an enquiry prior to a planning discussion, unless it is necessary for the protection of the adult at risk or others.
Enquiries are proportionate to the particular situation. The circumstances of each individual case determines the scope and who leads it. Enquiries should be outcome focussed, and best suit the particular circumstances to achieve the outcomes for the adult.
There is a statutory duty of co-operation and in most cases, there will be an expectation that enquiry will be made as requested. The statutory duty does not apply if co-operation would be incompatible with its own duties or would have an adverse effect on its own functions.
Local authorities and their relevant partners must respond to requests to cooperate under their general public law duties to act reasonably.
If an organisation declines to undertake an enquiry or if the enquiry is not done, local escalation procedures should be followed. The key consideration of the safety and wellbeing of the adult must not be compromised in the course of any discussions or escalation and it is important to emphasise that the duty to cooperate is mutual.
When planning an enquiry, a review should be made of:
- the adult’s mental capacity to understand the type of enquiry, the outcomes and the effect on their safety now and in the future
- whether consent has been sought
- whether an advocate or other support is needed
- the level and impact of risk of abuse and neglect
- the adults’ desired outcome
- the adult’s own strengths and support networks.
6.8 Communication and actions
It may be helpful to agree the best way to keep the adult and relevant parties informed. Where the enquiry is complicated and requires a number of actions that may be taken by others to support the outcome it may be appropriate for a multiagency enquiry meeting. Where enquiries are simple, single agency enquiries it may not be necessary to hold a meeting. Action should never be put on hold, due to the logistics of arranging meetings. Proportionality should be the guiding principle.
If the adult wishes to participate in meetings with relevant partners, one should be convened. Action, however, should not be ‘on hold’ until a meeting can be convened. If the adult does not have the capacity to attend, then an advocate should represent their views.
Good practice guide – Involving adults in safeguarding meetings
Effective involvement of adults and/or their representatives in safeguarding meetings requires professionals to be creative and to think in a person-centred way.
- How should the adult be involved?
- Where is the best place to hold the meeting?
- How long should the meeting last?
- Timing of the meeting?
- Agenda
- Preparation with the adult
- Who should chair?
- Agreement by all parties to equality
Information sharing should be timely, co-operation between organisations to achieve outcomes essential and action co-ordinated keeping the safety of the adult as paramount. Information sharing should comply with all legislative requirements.
Where one agency is unable to progress matters further, for example a criminal investigation may be completed but not necessarily achieve desired outcomes (e.g. criminal conviction), the local authority in consultation with the adult and others decide if and what further action is needed.
6.9 Support networks
The strengths of the adult at risk should always be considered. Mapping out with the adult and identifying their strengths and that of their personal network may reduce risks sufficiently so that people feel safe without the need to take matters further.
Any risk should be assessed and managed at the beginning of the enquiry and reviewed throughout.
6.10 Types of enquiries
| Types of enquiries | Who might lead |
|---|---|
| Criminal (including assault, theft, fraud, hate, crime, domestic violence and abuse or wilful neglect | Police |
| Domestic abuse (serious risk of harm) | Police chair the MARAC process and are supported by the MARAC coordinator and IDVAS |
| Anti-social behaviour (e.g. harassment, nuisance by neighbours) | Community safety services/local Policing (e.g. Safer Neighbourhood Teams). |
| Breach of tenancy agreement (e.g. harassment, nuisance by neighbours) | Landlord/registered social landlord/housing trust/community safety services |
| Bogus callers or rogue traders | Trading Standards/Police |
| Complaint regarding failure of service provision (including neglect of provision of care and failure to protect one service user from the actions of another) | Manager/proprietor of service/complaints department Ombudsman (if unresolved through complaints procedure) |
| Breach of contract to provide care and support | Service commissioner (e.g. Local Authority, NHS CCG) |
| Fitness of registered service provider | CQC |
| Serious Incident (SI) in NHS settings | Root cause analysis investigation by relevant NHS Provider |
| Unresolved serious complaint in health care setting | CQC, Health Service Ombudsman |
| Breach of rights of person detained under the MCA 2007 Deprivation of Liberty Safeguards (DoLS) | CQC, Local Authority, OPG/Court of Protection |
| Breach of terms of employment/disciplinary procedures | Employer |
| Breach of professional code of conduct | Professional regulatory body |
| Breach of health and safety legislation and regulations | HSE/CQC/Local Authority Link to – 2015 MoU |
| Misuse of enduring or lasting power of attorney or misconduct of a court appointed deputy | OPG/Court of Protection/Police |
| Inappropriate person making decisions about the care and wellbeing of an adult who does not have mental capacity to make decisions about their safety and which are not in their best interests | OPG/Court of Protection |
| Misuse of appointeeship or agency | DWP |
| SAR (Care Act Section 44) | Local SABs |
A range of options can also be found at the LGA website for making safeguarding personal.
Enquiries can range from non-complex single agency interventions to multi-agency complex enquiries. The key questions in choosing the right type of enquiry, is dependent on:
- what outcome does the adult want?
- how can enquiries be assessed as successful in achieving outcomes?
- what prevention measures need to be in place?
- how can risk be reduced?
Identifying the primary source of risk may assist in deciding what the most appropriate and proportionate response to the individual enquiry might be. There are no hard and fast rules and judgement will need to be made about what type of enquiry and actions are right for each particular situation.
6.10.1 Linking different types of enquiries
There are a number of different types of enquiries. It is important to ensure that where there is more than one enquiry that information is dovetailed to avoid delays, interviewing staff more than once, making people repeat their story.
Other processes, including police investigations, can continue alongside the safeguarding adult’s enquiry. Where there are HR processes to consider, it is important to ensure an open and transparent approach with staff, and that they are provided with the appropriate support, including trade union representation. The remit and authority of organisations need to be clear when considering how different types of investigations might support section 42(2) enquiries.
6.11 Enquiry reports
Once all actions have been completed a report should be collated and drawn up by the professional completing the safeguarding activities and the manager with oversight. Where there are contributions from other agencies/staff, these should be sent to the professional or manager within agreed formats and timeframes, so that there is one comprehensive report that includes all sources of information.
Reports need to be concise, factual and accurate. Reports should be drafted and discussed with the adult at risk/advocate. Reports need to address general and specific personalised issues. They should cover:
- views of the adult at risk
- whether outcomes were achieved
- is there evidence that section 42(2) criteria were met
- whether any further action is required and if so by whom
- who supported the adult and if this is an on-going requirement
In some enquiries, there will be an investigation for example, a disciplinary investigation, which may form part of the enquiry report. In drawing up the report, the risk assessment should be reviewed, and any safeguarding plan adjusted accordingly.
Recommendations should be monitored and taken forward. Agencies are responsible for carrying out the recommendations which might be included in future safeguarding plans.
6.11.1 Standards and analysis
The report should be tested to ensure that it meets the standards above, and analysed to assess whether there are gaps, contradictions and that information has been triangulated, i.e. is the report evidence based, and is there sufficient corroboration to draw conclusions.
The report and recommendations of the enquiry should be discussed with the adult at risk and or their advocate, who may have a view about whether it has been completed to a satisfactory standard.
Overall, the local authority should decide if the enquiry is completed to a satisfactory standard. In reaching this decision, the local authority may wish to consult partner organisations involved in the enquiry. If another organisation has led on the enquiry, the local authority may decide that a further enquiry should be undertaken by the local authority. The exception to this is where there is a criminal investigation, and, in this case, the local authority should consider if any other enquiry is needed that will not compromise action taken by the police.
6.12 Outcome to the enquiry
All enquiries should have established outcomes that determine the effectiveness of interventions. Decisions should be made whether:
- The adult has needs for care and support
- They were experiencing or at risk of abuse or neglect
- They were unable to protect themselves
- Further action should be taken to protect the adult from abuse or neglect
6.12.1 Evaluation by the adult at risk
- Were the desired outcomes met? (In exploring this, there is a need to clarify whether they were):
- Fully met
- Partially met
- Not met
- Do they feel safer?
- Yes
- Partially – in some areas but not others
- No
The evaluation is that of the adult, and not of other parties. Whilst staff may consider that enquiry and actions already taken have made the adult safe, and that their outcomes were met, the important factor is how actions have impacted on the adult. This should be clarified when assessing the performance of safeguarding.
6.12.2 Outcome for the person(s) alleged to have caused harm
To ensure the safety and wellbeing of other people, it may be necessary to take action against the person/organisation alleged to have caused harm. Where this may involve a prosecution, the police and the Crown Prosecution Service lead sharing information within statutory guidance.
The police may also consider action under the Common Law Police Disclosure (CLPD) which are the name for the system that has replaced the ‘Notifiable Occupations Scheme’. The CLPD addresses risk of harm regardless of the employer or regulatory body and there are no lists of specific occupations. The CLPD focusses on:
- disclosure where there is a public protection risk
- disclosures are subject to thresholds of ‘pressing social need’
- the ‘pressing social need’ threshold for making a disclosure under common law powers is considered to be the same as that required for the disclosure of non-conviction information by the DBS under Part V of the Police Act 1997 (as amended).
6.12.3 Support for people who are alleged to have caused harm
Where the person is also an adult who has care and support needs, organisations should consider what support and actions may help them not to abuse others. For example, enquiries may indicate that abuse was caused because the adult’s needs were not met and therefore a review of their needs should be made.
Where the person alleged to have caused harm is a carer, consideration should be given to whether they are themselves in need of care and support.
Checks might be made whether staff were provided with the right training, supervision and support. Whilst this does not condone deliberate intentions of abuse, prevention strategies to reduce the risk of it occurring again to the adult or other people should be considered.
When considering action for people who abuse, prevention and action to safeguard adults should work in tandem.
6.12.4 Recovery and resillience
Adults who have experienced abuse and neglect may need support to build up their resilience to move on from the incident. This support should enable people to use their own strengths and abilities to overcome what has happened, learn from the experience and develop an awareness that may prevent a reoccurrence. As a minimum it should enable people to recognise the signs and risks of abuse and neglect and know how to contact support if required.
Resilience is supported by recovery actions, which includes adults identifying actions that they would like to see to prevent the same situation arising. The process of resilience is evidenced by:
- the ability to make realistic plans and being capable of taking the steps necessary to follow through with them
- a positive perception of the situation and confidence in the adult at risks own strengths and abilities
- increasing their communication and problem-solving skills
Resilience processes that either promote well-being or protect against risk factors, benefits individuals and increases their capacity for recovery. This can be done through individual coping strategies assisted by:
- strong personal networks and communities
- social policies that make resilience more likely to occur
- handovers/referrals to other services for example care management, or psychological services to assist building up resilience
- restorative practice
If no further safeguarding action is required and there are alternative ways of supporting adults where they may be needed, then the section 42(2) enquiry can be closed down.
Actions and decisions under section (42 (2) enquiries
Actions
- plan the enquiry
- plan the enquiry
- identify professional to complete enquiry activities
- clarify desired outcomes
- identify links to other procedures in progress
- allocate agreed actions
- update safeguarding plan
- agree communication
- agree outcomes for person(s) alleged to have caused harm
- make referrals as agreed in relation to the person alleged to have caused harm
- make referrals in relation to the adult
- evaluation by the adult/advocate
- explore recovery and resilience
Manager who may allocate some of the actions to the professional completeing the enquiry activities.
Decisions
- what type of enquiry is appropriate and proportionate?
- who should contribute?
- does the report meet standards?
- necessary for the enquiry to be taken over by the local authority
- whether to close the enquiry down or take forward for review
- actions for the adult
- actions for the person alleged to have caused harm.
Manager in consultation with the adult and others.
Stage 3: Safeguarding plan and review

7.1 Safeguarding plan
In most cases there will be a natural transition between deciding what actions are needed and the end of the enquiry, into formalising what these actions are and who needs to be responsible for each action – this is the adult safeguarding plan.
An adult safeguarding plan is not a care and support plan, and it will focus on care provision only in relation to the aspects that safeguard against abuse or neglect, or which offer a therapeutic or recovery-based resolution. In many cases the provision of care and support may be important in addressing the risk of abuse or neglect, but where this is the intention the adult safeguarding plan must be specific as to how this intervention will achieve this outcome.
The safeguarding plan should set out:
- what steps are to be taken to assure the future safety of the adult at risk
- the provision of any support, treatment or therapy, including on-going advocacy
- any modifications needed in the way services are provided (e.g. same gender care or placement; appointment of an OPG deputy)
- how best to support the adult through any action they may want to take to seek justice or redress
- any on-going risk management strategy as appropriate.
The plan should outline the roles and responsibilities of all individuals and agencies involved and should identify a professional who will monitor and review the plan, and when this will happen. Adult safeguarding plans should be person-centred, and outcome focused. Safeguarding plans should be made with the full participation of the adult at risk. In some circumstances it may be appropriate for safeguarding plans to be monitored through ongoing care management responsibilities. In other situations, a specific safeguarding review may be required.
7.2 Review of the enquiry (optional)
The identified professional should monitor the plan on an on-going basis, within agreed timescales. The purpose of the review is to:
- evaluate the effectiveness of the adult safeguarding plan
- evaluate whether the plan is meeting/achieving outcomes
- evaluate risk
Reviews of adult safeguarding plans, and decisions about plans should be communicated and agreed with the adult at risk. Following the review process, it may be determined that:
- the adult safeguarding plan is no longer required
- the adult safeguarding plan needs to continue
Any changes or revisions to the plan should be made, new review timescales set (if needed) and agreement reached regarding the lead professional who will continue monitoring and reviewing; or, it may also be agreed, if needed, to instigate a new adult safeguarding section 42(2) Enquiry. New safeguarding enquiries will only be needed when the Local Authority determines it is necessary. If the decision is that further enquiries would be a disproportionate response to new or changed risks, further review and monitoring may continue.
Stage 4:Closing the enquiry
8.1 Closing the enquiry
Safeguarding can be closed at any stage. Individuals should be advised on how and who to contact with agreement on how matters will be followed up with the adult at risk if there are further concerns. It is good practice where a care management assessment, reassessment of care and support, health review, placement review or any other pre-booked review is due to take place following the safeguarding enquiry, for a standard check to be made that there has been no reoccurrence of concerns.
Closure records should note the reason for this decision and the views of the adult at risk to the proposed closure. The manager with oversight should ensure that all actions have been taken, building in any personalised actions:
- agreements with the adult at risk to closure and ensuring that the overarching duty to promote well-being has been considered
- referral for assessment and support
- advice and Information provided
- all organisations involved in the enquiry updated and informed
- feedback has been provided to the referrer
- all safeguarding records are full and proper and of a quality that meets organisational requirements, evidencing clear rationale for all decisions made
- action taken with the person alleged to have caused harm
- action taken to support other adults (if necessary)
- referral to children and young people made (if necessary)
- outcomes noted and evaluated by adult at risk
- consideration for a SAR
- any lessons to be learnt.
8.1.1 Closing enquiries down when other processes continue
The section 42(2) enquiry may be closed but other processes may continue, for example, a disciplinary or professional body investigation. These processes may take some time. Consideration may need to be given to the impact of these on the adult and how this will be monitored. Where there are outstanding criminal investigations and pending court actions, the section 42(2) enquiry can also be closed providing that the adult is safeguarded.
All closures no matter at what stage are subject to an evaluation of outcomes by the adult at risk. If the adult at risk disagrees with the decision to close the section 42(2) enquiry their reasons should be fully explored and alternatives offered.
At the close of each enquiry there should be evidence of:
- enhanced safeguarding practice ensuring that people have an opportunity to discuss the outcomes they want at the start of safeguarding activity
- follow-up discussions with people at the end of safeguarding activity to see to what extent their desired outcomes have been met
- recording the results in a way that can be used to inform practice and provide aggregated outcomes information for SABs
Appendix 1: Safeguarding adults structures and organisations
Roles and responsibilities
Local authorities
Local Authorities have statutory responsibility for safeguarding and are responsible for the public law decision as to whether or not to proceed with the duty to make enquiries under S42(2). Although the local authority is the lead agency for making enquiries, it may require others to undertake them. It is important that the most appropriate agency / person leads the enquiry to ensure that people are provided with the most appropriate support to meet their individual needs and are enabled to achieve positive outcomes. The specific circumstances will often determine who the right person is to begin an enquiry. In many cases a professional who already knows the adult will be the best person. The local authority retains the responsibility for ensuring that the enquiry is referred to the right place and is acted upon. The local authority should be clear about timescales, the need to know the outcomes of the enquiry and what action will follow if this is not done.
Local authority and NHS partnerships
‘Local Authorities can continue to enter into partnership arrangements with the NHS for the NHS to carry out a local authority’s ‘health-related functions’ (as defined in the 2000 Regulations [the NHS Bodies and Local Authorities Partnership Arrangements Regulations 2000l]). This effectively authorises NHS bodies to exercise those prescribed functions, including adult safeguarding functions. These arrangements are ‘partnership arrangements’ rather than ‘delegations’. In addition, by virtue of Regulation 4 of the 2000 Regulations, arrangements may only be entered into ‘if the partnership arrangements are likely to lead to an improvement in the way in which those functions are exercised’. The local authority would still remain legally responsible for how its functions (including adult safeguarding) are carried out via partnership arrangements.’ (Department of Health March 2015).
Within this guidance and procedure, where there are partnership agreements under Section 75 of the NHS Act 2006 with Mental Health Trusts, appropriately trained managers within the trust can act on behalf of the local authority to undertake adult safeguarding duties. Where this is done, the legal responsibility for safeguarding remains with the local authority.
Commissioners
Commissioners from the Clinical Commissioning Group, local authority and NHS England are all vital to promoting adult safeguarding. Commissioners have a responsibility to assure themselves of the quality and safety of the organisations they procure and ensure that contracts have explicit clauses that hold providers to account for preventing and dealing promptly with any concerns of abuse and neglect.
Health providers
All health providers are responsible for the safety and quality of services. Health providers are required to demonstrate that that they have safeguarding leadership, expertise and commitment at all levels. Health providers are required to have effective arrangements in place to safeguard adults at risk of abuse and neglect, and to assure themselves, regulators and their commissioners that these are effective and meet the required standards. Safeguarding arrangements mirror those of the Clinical Commissioning Group. Where appropriate the Clinical Commissioning Group (CCG) will support where there are concerns regarding the quality of enquiries delegated to NHS providers.
NHS England
The general function of NHS England is to promote a comprehensive health service to improve the health outcomes for people in England. NHS England has a statutory requirement to oversee assurance of Clinical Commissioning Groups (CCGs) in their commissioning role. The mandate from government sets out a number of objectives which NHS England is legally obliged to pursue. The objectives relevant to safeguarding are:
- continuing to improve safeguarding practice in the NHS
- ontributing to multi-agency family support services for vulnerable and troubled families
- contributing to reducing violence, in particular by improving the way the NHS shares information about violent assaults with partners and supports victims of crime.
NHS England is also responsible for ensuring, in conjunction with local CCG Clinical Leads, that there are effective arrangements for the employment and development of a named GP/named professional capacity for supporting primary care within the local area.
Care Quality Commission (CQC)
The CQC regulates and inspects health and social care services, including domiciliary services, and protects the rights of people detained under the Mental Health Act (1983). It has a role in identifying situations that give rise to concern that a person using a regulated service is or has been at risk of harm, or may receive an allegation or complaint about a service that could indicate potential risk of harm to an individual or individuals. The CQC should raise a safeguarding concern when appropriate to the safeguarding contact point.
Health and adult social care regulated services all have a key role in safeguarding vulnerable children and adults at risk. The CQC will monitor how these roles are fulfilled through its regulatory processes by assessing the quality and safety of care provided based on the things that matter to people. It does this using five key lines of enquiry to ensure that health and social care services provide people with safe, effective, caring, responsive and well led services. Specifically, it considers safeguarding within the ‘safe’ key line of enquiry.
The CQC will be directly involved with the safeguarding adults process where:
- one or more registered people are directly implicated
- urgent or complex regulatory action is indicated
- a form of enforcement action has commenced or is under consideration in relation to the quality of the service involved
Providers
All commissioned service provider organisations should produce their own guidelines that are consistent with the multiagency safeguarding adults guidance and local area procedures. These should set out the responsibilities of staff, clear internal reporting procedures, and clear procedures for reporting to the local safeguarding adults process. In addition, provider organisations’ internal guidelines should cover a whistleblowing policy which sets out assurances and protection for staff who raise concerns, how to work within best practice as specified in contracts, how to meet the standards in the Health and Social Care Act 2008 and the Care Quality Commission Regulations 2009, how to fulfil their legal obligations under statutory processes, robust recruitment arrangements, and training and supervision for staff.
The Voluntary or Community Sector (VCS)
Non-profit or not for profit sector organisations should include safeguarding adults within their induction programmes. Safeguarding should be integral to policies and procedures, for example:
- staff and volunteers are aware of what abuse is and how to spot it
- having a clear system of reporting concerns as soon as abuse is identified or suspected, with lead officers in place
- respond to abuse appropriately respecting confidentially
- prevent harm and abuse through rigorous recruitment and interview process
The VCS can promote safeguarding and support statutory organisations through consultations on policy, guidance and developments, work on prevention strategies and promoting wider public awareness.
The police
Although the police are a mandatory member of the SAB, they are not an agency responsible for the provision of care. The police role in adult safeguarding is related to their policing function. The core duties of the police are to prevent and detect crime, keep the peace, and protect life and property. The police are the lead on all criminal matters and must be consulted about any additional proposed action.
If you are concerned that an adult is in immediate danger or if there is a crime in progress involving an adult then contact the police on 999. If you believe that a criminal offence has occurred, but it is not in progress, and no one is in immediate danger, then contact police using 101 or report online. Professionals can also report safeguarding concerns to the Avon and Somerset Constabulary Lighthouse Safeguarding Unit. Please follow your internal policies relating to when to notify police about a death (typically when unexpected and/or suspicious circumstances).
The Coroner
Coroners are independent judicial office holders responsible for investigating violent, unnatural deaths or deaths of unknown cause, and deaths in custody or otherwise in state detention, which must be reported to them. The Coroner may have specific questions arising from the death of an adult at risk. These are likely to fall within one of the following categories:
- where there is an obvious and serious failing by one or more organisations
- where there are no obvious failings, but the actions taken by organisations require further exploration or explanation
- where a death has occurred and there are concerns for others in the same household or setting (such as a care home)
- deaths that fall outside the requirement to hold an inquest, but follow-up enquiries or actions are identified by the coroner or his/her officers.
Changes introduced through the Policing and Crime Act 2017 mean people who die while deprived of their liberty under the Deprivation of Liberty Safeguards (DoLS) or a Court of Protection order are no longer classed as having died in ‘state detention’. This means the deaths do not trigger an automatic requirement for an inquest.
Crown Prosecution Service (CPS)
The CPS is the principal public prosecuting authority for England and Wales and is headed by the Director of Public Prosecutions. Support is available within the judicial system to support adults at risk to enable them to bring cases to court and give best evidence. If a person has been the victim of abuse that is also a crime, their support needs can be identified by the police, the CPS and others who have contact with the adult at risk. Witness Care Units exist in all judicial areas and are run jointly by the CPS and the police.
Court of Protection
The Court of Protection deals with decisions and orders affecting people who lack capacity. The court can make major decisions about health and welfare, as well as property and financial affairs.
In most cases decisions about personal welfare will be able to be made legally without making an application to the court, as long as the decisions are made in accordance with the core principles set out in the Mental Capacity Act 2005 and the best interests checklist and any disagreements can be resolved informally. However, it may be necessary and desirable to make an application to the court in a safeguarding situation where there are:
- particularly difficult decisions to be made
- disagreements that cannot be resolved by any other means
- on-going decisions needed about the personal welfare of a person who lacks capacity to make such decisions for themselves
- matters relating to property and/or financial issues to be resolved
- serious healthcare and treatment decisions, for example, withdrawal of artificial nutrition or hydration
- concerns that a person should be moved from a place where they are believed to be at risk
Concerns or a desire to place restrictions on contact with named individuals because of risk or where proposed adult safeguarding actions may amount to a deprivation of liberty outside of a care home or hospital.
The Office of the Public Guardian (OPG)
The OPG was established under the Mental Capacity Act 2005 to support the public guardian and to protect people lacking capacity by:
- setting up and managing separate registers of lasting powers of attorney, and of court- appointed deputies
- supervising deputies
- sending court of protection visitors to visit individuals who lack capacity and also those for whom it has formal powers to act on their behalf
- receiving reports from attorneys acting under lasting powers of attorney and deputies
- providing reports to the court of protection
- dealing with complaints about the way in which attorneys or deputies carry out their duties.
The OPG can carry out an investigation into the actions of a deputy, of a registered attorney (lasting powers of attorney or enduring powers of attorney) or someone authorised by the court of protection to carry out a transaction for someone who lacks capacity, and report to the public guardian or the court.
Environmental Health
Environmental Health is responsible for health and safety enforcement in businesses, investigating food poisoning outbreaks, pest control, noise pollution and issues related to health and safety. Local authorities are responsible for the enforcement of health and safety legislation in shops, offices, and other parts of the service sector.
Trading Standards
From an adult safeguarding perspective trading standards services have a key role in safeguarding focus and should be protecting victims of scams and rogue traders. This includes both promoting awareness of, and disrupting, these types of criminal activity and working with partners to prosecute offenders when identified. Trading Standards also provide advice for businesses and is responsible for enforcing laws covering the safety, descriptions and pricing of products and services.
Educational settings
Although local authorities and the police hold the lead responsibility for responding to allegations of abuse in relation to adults and coordinating the local inter-agency framework for safeguarding adults, educational settings should assure the safe and secure provision for children, young people and learners. Safeguarding the welfare of children, young people and some vulnerable adult learners is part of their core business, and all staff should be aware of their responsibilities in this regard. Other agencies should alert educational settings of any concerns and ensure they are included in the safeguarding response.
Housing
The Care Act 2014 states that a local authority must consider cooperating with social housing providers in order to exercise its care and support duties. An authority must do this in particular when protecting adults at risk of harm and neglect and when identifying and sharing lessons to be learned from cases of serious abuse or neglect.
Social housing providers are registered with, and regulated, by the Homes England. They are also known as Registered Providers of Social Housing (RPs) or Registered Social Landlords (RSLs). They include local authority landlords, Arm’s-Length Management Organisations (ALMOs) that manage council housing stock, private for-profit or not-for-profit housing providers, and voluntary sector providers such as alms houses. Most not-for-profit RPs are also known as housing associations.
RPs provide a wide range of housing and housing-related services. They provide much of the supported accommodation in England, such as sheltered housing, care homes, supported living scheme housing, extra care schemes, hostels, foyers for young people, domestic abuse refuges, etc.
Beyond the core service of providing housing, RPs may also engage in initiatives that enhance their customers’ wellbeing and create sustainable communities, such as: housing support, community safety, better neighbourhoods, responding to antisocial behaviour, employment and training, domestic abuse, self-neglect and hoarding, fraud awareness, debt and financial inclusion, reducing isolation, tenancy sustainment support, etc. local authorities must take into account that the suitability of accommodation is a core component of wellbeing and good housing provision can variously promote that wellbeing. This includes minimising the circumstances, such as isolation, which can make some adults more vulnerable to abuse or neglect in the first place.
The nature and diversity of RPs’ work, therefore, can mean that their staff are often well placed to:
- have a good knowledge of the individual and the communities with whom they work
- be working with persons who are unable to protect themselves from abuse or neglect due to their care and support needs, but who are not already known to adult social care services
- identify individuals experiencing or at risk of abuse or neglect and raise concerns
- be the first professionals to whom individuals might first disclose abuse or neglect concerns
- be the only professionals working with the adult at risk
- provide essential information and advice regarding the adult at risk
- contribute actively to person-led safeguarding risk assessments and arrangements to support and protect an individual, where appropriate
- carry out a safeguarding enquiry, or elements of one
- work with agencies to support someone who is hoarding
- work together with agencies to resolve issues with someone who refuses support or self-neglects, or when someone may not be eligible for a safeguarding service or social care support
- work with local authorities to promote safeguarding awareness, information and prevention campaigns
- be instrumental in helping a local authority to successfully exercise its safeguarding and well-being duties
Housing providers should ensure that they develop a safeguarding culture through:
- board and leadership commitment and ownership of safeguarding responsibilities
- policies or guidance that promote the 6 principles of adult safeguarding
- policies that reflect the adult safeguarding framework set out by a SAB
- staff being vigilant about adult safeguarding concerns
- learning and development for staff on adult safeguarding and the Mental Capacity Act 2005 enabling them to fulfil their roles and responsibilities
- sharing information appropriately to safeguard adults at risk and engaging with Information Sharing Agreements where required
- developing inter-housing networks as well as multi-agency mechanisms
Prisons
The Care Act (2014) does not give legal authority to local authorities to carry out safeguarding enquiries where a prisoner with care and support needs may have been or has been at risk of abuse or neglect. SABs and local authority safeguarding teams can give advice and support on safeguarding to prison governors and other prison staff. Prisons and approved premises, like hospitals and care homes, are required to have their own internal safeguarding arrangements to respond to safeguarding concerns arising in prisons and they retain the responsibility for the safety of their detainees.
The National Offender Management Service has produced a policy document named Adult Safeguarding in Prisons to which prisons adhere to.
Community Rehabilitation Companies (CRC)
Since 1 June 2014 the delivery of Probation Services has been carried out by the National Probation Service (NPS) and Community Rehabilitation Companies (CRC). NPS are responsible for supervising high and very high risk of serious harm offenders on licence and community orders, and/ or those subject to Multi-Agency Public Protection Arrangement (MAPPA), preparing pre-sentence reports for courts, preparing parole reports, supervising offenders in approved premises, and delivering sex offender treatment programmes, support to victims of serious violent and sexual offences through the Victim Liaison Unit.
The CRC are responsible for supervising low and medium risk of serious harm offenders on licence and community orders, community payback, accredited programmes and other interventions. Both services have a remit to demonstrate a continuous focus on assessment and risk of harm, to protect adults at risk, children and young people, and victims of crime. One of their key objectives is to evidence that routine checks are completed (with appropriate agencies) and information accessed is used to inform the assessment and management of risk in all cases. The NPS works in partnership with other agencies through the Multi Agency Public Protection Arrangements (MAPPA). The purpose of the MAPPA framework is to reduce the risks posed by sexual and violent offenders in order to protect the public. The responsible authorities in respect of MAPPA are the police, prison and the NPS service that have a duty to ensure that a local MAPPA is established and the risk assessment and management of all identified MAPPA offenders is addressed through multi-agency working.
Although not a statutory requirement, representation from the NPS and CRC on the SAB should be considered.
Healthwatch
Healthwatch is the consumer champion in health and care and must be consulted on the Safeguarding Adult Partnership’s strategic plan. It operates at both local and national levels (Healthwatch England) and has significant statutory powers to ensure the voice of the consumer is strengthened. It challenges and holds to account commissioners, the regulators and providers of health and social care services. It identifies common problems with health and social care based on people’s experiences, recommends changes they know will benefit people, and holds services and decision-makers to account and demands action. As a statutory watchdog, its role is to ensure that health and social care services, and the government, put people at the heart of their care.
Health and wellbeing boards
The Health and Social Care Act 2012 establishes health and wellbeing boards as a forum where key leaders from the health and care system work together to improve the health and wellbeing of their local population and reduce health inequalities. They are an important feature of the NHS reforms and are key to promoting greater integration of health and local government services. Boards strike a balance between status as a council committee and role as a partnership body.
Local Safeguarding Children Board (LSCB)
Section 13 of the Children Act 2004 requires each local authority to establish a LSCB for their area and specifies the organisations and individuals (other than the local authority) that should be represented on the LSCBs. The police and health are core members of both the LSCB and the SAB. Working together to safeguard children 2018 removed the requirement to establish LSCBs on local authorities, and replaces it with a requirement that the three safeguarding ‘partners’ in an area (local authorities with children’s social care responsibilities, Clinical Commissioning Group(s) and police) establish new local arrangements from September 2019. Please refer to information published by your LSCB on arrangements from September 2019 for further information and guidance.
Quality Surveillance Groups (QSG)
QSGs are primarily concerned with NHS commissioned services, those services funded by the NHS including relevant public services. There are strategic links between SABs and QSGs. The QSGs are supported by NHS England. They provide an open forum for local supervisory, commissioning and regulatory bodies to share intelligence and give the opportunity to coordinate actions to ensure improvements in services. Its purpose is to ensure quality by early identification of risk.
Local Safeguarding Adult Board (LSAB)
All Local Authorities must establish a SAB as set out in the Care Act 2014. The Act (Schedule 2) gives the local SAB three specific duties it must do:
- publish a strategic plan for each financial year that sets out how it will meet its main objective and what each member is to do to implement that strategy. In developing the plan it must consult the local healthwatch organisation and involve the community.
- publish an annual report detailing what the SAB has done during the year to achieve its objective and what it and each member has done to implement its strategy as well as reporting the findings of any SARs including any ongoing reviews
- decide when a SAR is necessary, arrange for its conduct and if it so decides, to implement the findings.
Senior strategic roles, strategic
The Care Act 2014 prescribes that each SAB should include the local authority, the Clinical Commissioning Group and the police.
Each SAB member agency should appoint a senior manager to take the lead strategic and inter-agency role in safeguarding arrangements, including the SAB. Within each partner agency, clearly understood roles should be created for practice leadership in safeguarding.
Principal Social Workers are well-placed to provide professional leadership and to provide additional advice and guidance to social workers in complex and contentious cases.
Healthcare providers should have in place named professionals to provide additional advice and support in complex and contentious cases within their organisations.
There should be a designated professional lead within the CCG, to act as the lead in the management of complex cases and to provide advice and support to the governing body.
Arrangements should be made to enable officers investigating safeguarding concerns to access advice from specially trained investigators and/or units within the police.
Glossary and acronyms
In using this guidance, a number of phrases, wording or acronyms have been used. The following provides more information and, where necessary, a definition:
Adult at risk is a person aged 18 or over who has needs for care and support (whether or not the local authority is meeting any of those needs), is experiencing, or at risk of abuse or neglect, and as a result of those care and support needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect.
Adult safeguarding means protecting a person’s right to live in safety, free from abuse and neglect.
Advocacy is supporting a person to understand information, express their needs and wishes, secure their rights, represent their interests and obtain the care and support they need.
Appropriate individual within this document an ‘appropriate individual’ is a person who supports an adult at risk typically but not exclusively in an advocacy role and is separate to an Appropriate Adult.
Best Interest – the Mental Capacity Act 2005 states that if a person lacks mental capacity to make a particular decision then whoever is making that decision or taking any action on that person’s behalf must do so in the person’s best interest. This is one of the principles of the MCA.
Care setting is where a person receives care and support from health and social care organisations. This can include a persons’ own home, hospitals, hospices, respite units, nursing homes, residential care homes, and day opportunities arrangements.
Carer – the Association of Directors of Adult Social Services (ADASS) define a carer as someone who ‘spends a significant proportion of their time providing unpaid support to a family member, partner or friend who is ill, frail, disabled or has mental health or substance misuse problems’.
Commissioning is the cyclical activity, to assess the needs of local populations for care and support services, determining what element of this, needs to be arranged by the respective organisations, then designing, delivering, monitoring and evaluating those services.
Concern is the term used to describe when there is or might be an incident of abuse or neglect and it replaces the previously used term of ‘alert’.
Contracting is the means by which a process is made legally binding. Contract management is the process that then ensures that services continue to be delivered to the agreed quality standards.
Disclosure and Barring Service (DBS) helps employers make safer recruitment decisions and prevent unsuitable people from working with vulnerable groups. It replaces the Criminal Records Bureau (CRB) and Independent Safeguarding Authority (ISA).
Enquiry establishes whether any action needs to be taken to stop or prevent abuse or neglect, and if so, what action and by whom the action is taken. The enquiry will be allocated to a professional to complete the safeguarding activity and there will be a Manager with oversight of the enquiry process.
Equality Act 2010 legally protects people from discrimination in the workplace and in wider society. It replaced previous anti-discrimination laws with a single Act, making the law easier to understand and strengthening protection in some situations. It sets out the different ways in which it is unlawful to treat someone.
General Data Protection Regulation (GDPR) is a legal framework that sets guidelines for the collection and processing of personal information of individuals within the European Union (EU). The GDPR sets out the principles for data management and the rights of the individual, while also imposing fines that can be revenue-based. The GDPR came into effect across the EU on May 25, 2018 and its requirements are part of English law under the Data Protection Act 2018.
Independent Domestic Violence Advisor (IDVA) – Adults who are the subject of domestic violence may be supported by an IDVA. IDVAs provide practical and emotional support to people who are at the highest levels of risk. Practitioners should consult with the adult at risk to consider if the IDVA is the most appropriate person to support them and ensure their eligibility for the service.
Independent Mental Capacity Advocate (IMCA) – established by the Mental Capacity Act (MCA) 2005 IMCAs are mainly instructed to represent people who lack capacity where there is no one else, such as family or a friend, who is able to support and represent them independently. IMCAs are a legal safeguard for people who lack the mental capacity to make specific important decisions about where they live, serious medical treatment options, care reviews or adult safeguarding concerns.
Independent Mental Health Advocate (IMHA) – under the Mental Health Act 1983 certain people known as ‘qualifying patients’ are entitled to the help and support from an Independent Mental Health Advocate. If there is a safeguarding matter whilst the IMHA is working with the adult at risk, consideration for that person to be supported by the same advocate should be given.
Independent Sexual Violence Advocate (ISVA) – is trained to provide support to people in rape or sexual assault cases. They help victims to understand how the criminal justice process works and explain processes, for example, what will happen following a report to the police and the importance of forensic DNA retrieval.
Making Safeguarding Personal (MSP) is about person centred and outcome focussed practice. It is how professionals are assured by adults at risk that they have made a difference to people by taking action on what matters to people and is personal and meaningful to them.
Multi-Agency Public Protection Arrangements (MAPPA) are a set of arrangements to manage the risk posed by the most serious sexual and violent offenders (MAPPA-eligible offenders) under the provisions of sections 325 to 327B of the Criminal Justice Act 2003.
Natural justice refers to the principles and procedures that govern the adjudication of an issue, which should be unbiased, without prejudice, and there is equal right to being heard.
Person/organisation alleged to have caused harm is the person/organisation suspected to be the source of risk to an adult at risk.
Procurement is the specific function to buy or acquire services which commissioners have duties to arrange to meet people’s needs, to agreed quality standards, providing value for money to the public purse.
Public Interest Test refers to the test used under data protection legislation when deciding whether the public interest in disclosing information in order to protect an adult at risk justifies interfering with the individual’s right to privacy.
Regulated Provider is an individual, organisation or partnership that carries on activities that are specified in Schedule 1 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014.
Safeguarding Adults Practice Lead/ Lead Practitioner is the title given to the member of staff in an organisation who is given the lead in the context of Professional Practice, advice and support to operational teams. In Torbay there is a Head of Safeguarding who has professional accountability and oversight for all Safeguarding Adults Operations.
Safeguarding Adults Team Manager (SATM) within Devon County Council this is a person who manages Devon County Council Safeguarding Adult Hubs, providing guidance and oversight of safeguarding adult concerns that are raised to the local authority.
Safeguarding Adult Reviews (SARs) are part of SABs statutory duty. A SAR is undertaken where an adult in its’ area dies as a result of abuse or neglect, whether known or suspected and there is concern that partner agencies could have worked more effectively to protect the adult. SABs must also arrange a SAR if an adult in its’ area has not died, but the SAB knows or suspects that the adult has experienced serious abuse or neglect.
Safeguarding Practitioner (Professionally Qualified Practitioner) is a member of staff who undertakes the actions to meet the overarching purpose of the section 42 (2) enquiry.
Strategic Executive Information System (StEIS) – Reporting a Serious Incident must be done by recording the incident on this system, which facilitates the reporting of serious incidents and the monitoring of investigations between NHS providers and commissioners.
Torbay and Devon Safeguarding Adults Partnership (TDSAP) – Safeguarding Adults Boards (SABs) were founded in 2014 as a requirement of the Care Act 2014 and provide strategic leadership for adult safeguarding. The TDSAP is the collective name for the partners that work with the board to safeguard adults across Torbay and Devon.
Vital interest a term used in the General Data Protection Regulation (GDPR) to permit sharing of information where it is critical to prevent serious harm or distress, or in life-threatening situations.
Acknowledgements
With thanks to London Safeguarding Adult Board, whose multiagency adult safeguarding policy and procedures have been adapted to produce this guidance.